CJC-1295 is one of the most frequently discussed growth-hormone-releasing hormone (GHRH) analogs in peptide research, yet the name is used loosely to describe two chemically distinct molecules with very different behavior in the body. The central research question this article addresses is straightforward but often muddled: what actually is CJC-1295, how does the “DAC” modification change its pharmacology, and what does the real published evidence — as opposed to marketing copy — tell us about its effects on growth hormone and IGF-1? This is an educational overview of the mechanism and the literature, written for a research and reference context. Nothing here is medical advice, and CJC-1295 in either form is not an FDA-approved therapeutic drug for human use.
Below, we separate the two compounds that share the “CJC-1295” label, explain the albumin-binding chemistry that gives the DAC version its multi-day half-life, walk through the GHRH-receptor mechanism, and then look honestly at how thin the human evidence base really is. Where a claim rests on preclinical or mechanistic reasoning rather than human trials, we say so plainly.
What is CJC-1295?
CJC-1295 is a synthetic analog of growth-hormone-releasing hormone (GHRH), the hypothalamic peptide that signals the anterior pituitary to synthesize and release growth hormone (GH). Native human GHRH is a 44-amino-acid peptide, but its biological activity is concentrated in the first 29 residues — the fragment GHRH(1–29), which retains essentially full potency and is the basis for the drug sermorelin. CJC-1295 is built on this GHRH(1–29) backbone.[5]
The compound was developed in the mid-2000s by ConjuChem Biotechnologies, a Canadian company whose platform centered on extending peptide half-lives by tethering them to circulating serum albumin. In the scientific literature the DAC-bearing molecule was originally designated DAC:GRF (drug affinity complex : growth-hormone-releasing factor). Its formal modification nomenclature is often written as N-epsilon-30-maleimidopropionyl-[D-Ala2, Gln8, Ala15, Leu27]-Sermorelin-Lys30 — a description that encodes both the four amino-acid substitutions and the albumin-binding appendage.[5]
The four amino-acid substitutions
Native GHRH(1–29) is degraded extremely quickly in plasma — some reports place its functional half-life at only a few minutes — largely because the enzyme dipeptidyl peptidase-IV (DPP-IV) cleaves it near the N-terminus, and other peptidases attack additional sites. To harden the peptide against this, CJC-1295’s backbone carries four amino-acid substitutions relative to the native sequence, at positions 2, 8, 15 and 27 (commonly D-Ala2, Gln8, Ala15, Leu27). This is why the peptide is sometimes called “tetrasubstituted GRF(1–29).” The substitution at position 2 in particular blunts DPP-IV cleavage, while the others improve resistance to other proteases and can enhance receptor affinity and manufacturing stability.[5]
The position-2 change is worth dwelling on, because it is the same principle that underlies several modern peptide drugs. DPP-IV (also called CD26) is a membrane-bound serine protease that snips a two-amino-acid fragment off the N-terminus of any peptide bearing a proline or alanine at position 2. In native GHRH and in sermorelin, DPP-IV cleaves the bond right after the second residue, producing the fragment GRF(3–29), which can no longer bind the GHRH receptor — the peptide is inactivated almost as fast as it enters the blood. Substituting a D-alanine (the mirror-image stereoisomer) at position 2 makes that bond a poor substrate for the enzyme, because DPP-IV’s active site is stereospecific and does not accommodate the D-configuration well. Classic enzymology on GHRH-family peptides showed just how sensitive cleavage is to what sits at position 2, with certain substitutions dropping the hydrolysis rate to a small fraction of the native peptide’s.[10] The three remaining substitutions (at 8, 15 and 27) further reduce susceptibility to other proteases and improve the molecule’s stability during manufacturing and storage, all while leaving the receptor-binding pharmacophore essentially intact.
This tetrasubstituted backbone, on its own — without any albumin-binding component — is the molecule most people mean when they say “CJC-1295 no-DAC,” and it is chemically the same entity marketed under the name Modified GRF(1–29) or Mod GRF(1–29). It is important to hold onto this point because it is the single largest source of confusion around CJC-1295: the “with-DAC” and “no-DAC” products are not two doses of the same thing, they are two different molecules with roughly a hundred-fold difference in duration of action.
A note on the confusing nomenclature
Much of the muddle in this area is purely a naming problem. Strictly speaking, the original ConjuChem designation “CJC-1295” referred to the DAC-bearing long-acting molecule (DAC:GRF). The short-acting tetrasubstituted backbone that lacks the DAC was, in the primary literature, more properly called Modified GRF(1–29). Over time, the research-peptide market began labeling that short-acting backbone as “CJC-1295 without DAC” or “CJC-1295 no-DAC,” effectively retrofitting the CJC-1295 brand onto a molecule that arguably should keep the Mod GRF(1–29) name. The result is that a single label — “CJC-1295” — is now used for two compounds whose durations differ by two orders of magnitude. Whenever you read about “CJC-1295,” the first question to ask is always: with DAC or without? The answer changes almost everything downstream, from half-life to injection frequency to the shape of the GH response.
What does “DAC” mean, and how does it extend half-life?
DAC stands for Drug Affinity Complex, the ConjuChem technology that gives the long-acting version its name. The concept is to attach a small reactive chemical “handle” to the peptide so that, once injected, the peptide covalently latches onto a long-lived carrier protein already circulating in the blood: human serum albumin.[5]
The maleimide–Cys34 bond
In CJC-1295 with DAC, a maleimidopropionic-acid group is attached via a lysine residue appended at position 30, just beyond the core 29-amino-acid sequence. Maleimide is a chemical group that reacts selectively and rapidly with free thiol (sulfhydryl) groups. Human serum albumin, the most abundant protein in plasma, carries one notably reactive free thiol at cysteine-34 (Cys34). After subcutaneous injection, the maleimide on CJC-1295 forms a stable covalent thioether bond with albumin’s Cys34, essentially fusing the peptide to a protein whose own half-life in humans is on the order of two to three weeks.[5]
The consequences of this bond are large. A small peptide is normally cleared within minutes to hours by enzymatic degradation and renal filtration. Once bound to albumin, the peptide is shielded from peptidases and is too large to be filtered by the kidney, so it persists as albumin persists. This is the mechanism that turns a peptide with a native half-life of roughly half an hour into one that measurably stimulates the GH axis for many days after a single dose. The same albumin-binding strategy underlies other ConjuChem constructs, and CJC-1295’s DAC handle was designed to bind albumin in the bloodstream after injection rather than requiring a pre-formed conjugate.[5]
Why albumin, specifically?
Albumin is an unusually good carrier for this trick for several reasons. It is the most abundant protein in plasma, so there is always plenty of it available to capture an injected DAC peptide. It circulates for a long time — roughly two to three weeks in humans — because it is recycled rather than rapidly degraded, in part through a salvage pathway involving the neonatal Fc receptor. And it happens to carry that single, unusually reactive free thiol at Cys34, which most other abundant plasma proteins lack. The maleimide chemistry exploits exactly that one reactive site, so the peptide preferentially ends up on albumin rather than reacting nonspecifically all over the proteome. In effect, the DAC design borrows albumin’s long lifespan and hands it to a small peptide that would otherwise be gone in half an hour. This is the same broad rationale — hijacking a long-lived carrier — used by several albumin-binding drug technologies, though the specific maleimide–Cys34 approach is characteristic of the ConjuChem platform.
What the DAC does not change
A crucial point of honesty: attaching a peptide to albumin changes its pharmacokinetics (how long it lasts), not its pharmacology at the receptor. The GHRH-receptor-binding part of the molecule is the same tetrasubstituted GRF(1–29) core in both forms. So the DAC does not make CJC-1295 “stronger” per molecule at the receptor; it makes each molecule last far longer, which converts a series of sharp pulses into a sustained plateau of stimulation. That distinction — duration, not intrinsic potency — is the correct mental model for the whole with-DAC-versus-no-DAC debate.
CJC-1295 DAC vs no-DAC (Mod GRF 1-29): how do they compare?
The two forms share the same tetrasubstituted GHRH(1–29) core and act on the same receptor. The difference is entirely in duration and, consequently, in the pattern of GH release they produce. The no-DAC form (Mod GRF 1-29) is short-acting, with a reported half-life in the range of about 30 minutes — long enough to drive a single, physiologic-looking GH pulse and then clear. The DAC form binds albumin and produces a prolonged, low-level elevation of GH and IGF-1 that the community often calls a “GH bleed,” lasting days rather than minutes.
| Attribute | CJC-1295 with DAC | CJC-1295 no-DAC (Mod GRF 1-29) |
|---|---|---|
| Molecular basis | Tetrasubstituted GRF(1–29) + maleimide/Lys30 albumin-binding appendage | Tetrasubstituted GRF(1–29) only |
| Approximate half-life | ~6–8 days (albumin-bound) | ~30 minutes |
| GH release pattern | Sustained, prolonged elevation (“bleed”); blunts natural pulsatility | Short, discrete pulse that more closely mimics endogenous GHRH |
| IGF-1 effect (in research) | Elevated for many days after a single dose; can accumulate with repeat dosing | Shorter-lived, pulse-associated changes |
| Frequency studied in research settings | Infrequent administration (e.g., weekly-type intervals in animal work) | More frequent administration to reproduce repeated pulses |
| Published human evidence | One key single-dose PK/PD study (Teichman 2006) plus a preclinical base | Very limited; little dedicated published human trial data |
For a deeper, protocol-level breakdown of the two forms and how each is handled in a research context, see the CJC-1295 no-DAC 5 mg research protocol and the companion CJC-1295 DAC 5 mg research protocol. These pages describe reconstitution and handling conventions, not human dosing advice.
How does CJC-1295 work?
CJC-1295, like all GHRH analogs, works by engaging the GHRH receptor (GHRH-R) on the pituitary somatotrophs — the specialized cells of the anterior pituitary that make and store growth hormone. The GHRH receptor is a class-B (secretin-family) G-protein-coupled receptor with seven transmembrane domains, expressed primarily on these somatotrophs.[3]
From receptor binding to GH release
When a GHRH agonist binds GHRH-R, the receptor couples to the stimulatory G-protein (Gs), which activates adenylate cyclase and raises intracellular cyclic AMP (cAMP). This rise in cAMP is the initiating event of GHRH-driven GH secretion. Elevated cAMP activates protein kinase A (PKA), which phosphorylates the transcription factor CREB; phosphorylated CREB in turn drives transcription of the GH gene and helps sustain the somatotroph-specific transcription factor Pit-1. In parallel, the signaling cascade promotes membrane depolarization and opening of voltage-sensitive calcium channels, and the resulting calcium influx triggers the exocytosis of GH stored in secretory granules.[3]
So GHRH signaling does two things at once: it releases the GH that is already made and stored, and it drives the synthesis of new GH to refill the stores for the next pulse. This dual role matters for understanding the difference between the DAC and no-DAC forms.
Downstream: GH to IGF-1
Once released into the circulation, GH acts on the liver and other tissues to stimulate production of insulin-like growth factor 1 (IGF-1). IGF-1 mediates many of the anabolic and growth-related effects attributed to the GH axis and has a far more stable blood level than GH itself, which is why researchers so often use IGF-1 as the readout of sustained GHRH-analog activity. When you read that CJC-1295 with DAC “raises IGF-1 for over a week,” IGF-1 is functioning as the durable biomarker of the prolonged GH stimulation.
Pulsatile versus sustained signaling
Endogenous GH secretion is pulsatile — sharp bursts separated by troughs, sculpted by the opposing hypothalamic hormones GHRH (stimulatory) and somatostatin (inhibitory). The short-acting no-DAC form, clearing in roughly half an hour, produces a discrete pulse and then allows the natural trough to return, which more closely resembles physiologic signaling. The DAC form, by contrast, keeps GHRH-R stimulation switched on for days, producing a flatter, more continuous elevation rather than clean pulses. Whether continuous “always-on” GHRH signaling is desirable or not is one of the genuinely open questions in this area, because the natural system is built around pulsatility and negative feedback. The GHRH receptor and its signaling are reviewed in the endocrinology literature.[3] Readers who want plain-language definitions of terms like somatotroph, secretagogue and pulsatility can consult the peptide research glossary.
The role of somatostatin and IGF-1 feedback
To understand why a long-acting GHRH signal behaves differently from a short pulse, you have to bring in the two brakes on the system. The first is somatostatin, the hypothalamic hormone that inhibits GH release; the natural GH pulse pattern emerges from the interplay of GHRH pushing and somatostatin pulling on the same somatotrophs. The second is IGF-1 negative feedback: as GH rises and drives IGF-1 up, the elevated IGF-1 feeds back on the hypothalamus, stimulating somatostatin release and thereby damping further GH secretion. Classic human physiology work demonstrated that IGF-1 infusion suppresses GH mainly by blunting the amplitude of spontaneous GH pulses, and that this suppression operates through hypothalamic somatostatin.[11]
This feedback loop is exactly why the DAC form cannot simply produce “more and more” GH indefinitely. As a continuous GHRH signal drives IGF-1 up and keeps it up for days, the rising IGF-1 recruits somatostatin, which in turn opposes the very GH release the peptide is trying to provoke. The system is self-limiting. It is one reason the observed GH elevations in the human study were substantial but bounded (a few-fold, not orders of magnitude), and it is a reason to be skeptical of claims that continuous GHRH stimulation can override the body’s regulatory ceiling. A GHRH analog nudges an intact, self-correcting axis; it does not seize control of it.
The “GH bleed” and why pattern matters
Researchers and the peptide community often describe the DAC form as producing a “GH bleed” — a low-grade, continuous seepage of GH rather than clean pulses. The distinction between a pulse and a bleed is not cosmetic. A great deal of GH biology is thought to depend on the pattern of exposure, not just the total amount: pulsatile GH and continuous GH can produce different downstream gene-expression and metabolic effects in target tissues, which is one reason natural secretion is so tightly pulsatile in the first place. This is precisely why some researchers prefer the short-acting no-DAC form when the goal is to reproduce a physiologic pulse, and why the long-term consequences of the DAC form’s sustained pattern in humans remain an open question rather than a settled benefit.
What does the human research actually show?
This is where honesty matters most. Despite the enormous volume of online writing about CJC-1295, the dedicated human clinical literature is small. The single most important human study is Teichman and colleagues, published in the Journal of Clinical Endocrinology & Metabolism in 2006.[1]
The Teichman 2006 study
Teichman et al. conducted a randomized, double-blind, placebo-controlled Phase 1 study of CJC-1295 with DAC in healthy adults. Participants received single subcutaneous doses across a dose range, and the investigators tracked GH and IGF-1 over time. The key findings were:
- A single subcutaneous injection produced dose-dependent increases in mean plasma GH of roughly 2- to 10-fold, sustained for six days or more.
- Mean plasma IGF-1 rose by about 1.5- to 3-fold above baseline and remained elevated for approximately 9 to 11 days after that single dose.
- With repeated dosing, IGF-1 elevation could be maintained on the order of several weeks.
- The compound was described as safe and relatively well tolerated over the doses studied in this short-term setting.
This study is the empirical foundation for essentially every claim about CJC-1295 DAC’s multi-day duration. It cleanly demonstrated that the albumin-binding strategy works in humans: one shot, and the GH/IGF-1 axis stays elevated for well over a week.[1]
The honest limits of that evidence
It is equally important to state what Teichman 2006 does not establish:
- It is a short-term pharmacodynamic study in healthy volunteers, not a trial of any clinical outcome. It measured hormone levels, not body composition, strength, recovery, injury healing, longevity, or any of the benefits commonly claimed online.
- It studied the DAC form. The no-DAC / Mod GRF(1–29) form does not have a comparable, well-known dedicated human pharmacokinetic trial in the published literature; its human profile is largely inferred from its short half-life and from the broader GHRH-analog class.
- It was a single study with a modest number of participants, not a body of replicated randomized controlled trials.
The preclinical foundation
Beyond the human study, much of the mechanistic confidence in CJC-1295 comes from animal work. In a frequently cited experiment, one-week-old mice genetically lacking GHRH (a knockout model that grows poorly precisely because it cannot signal its own pituitary) were treated for five weeks with CJC-1295 at intervals of 24, 48 or 72 hours. Animals receiving the drug every 24 hours grew to normal body weight and length, effectively rescuing the phenotype. Spacing the injections further apart — every 48 or 72 hours — still improved growth relative to placebo but failed to fully normalize it, while lean-mass and body-composition measures were preserved across the treated groups.[2]
This is genuinely informative biology: it confirms that CJC-1295 engages the GHRH axis in a living animal well enough to drive normal growth, and it hints that dosing interval matters. But two caveats belong in the same breath. First, it is a mouse model of GHRH deficiency — a system with no baseline GHRH being handed a replacement — which is not the same as adding a long-acting GHRH signal on top of an already-normal human axis. Second, it measured growth in developing animals, not any outcome of interest to an adult human. It supports the mechanism; it does not establish a human benefit.
The correct way to read the evidence base overall is: one solid human PK/PD study on the DAC form, a supporting preclinical foundation, and a large gap where clinical-outcome trials would be. Everything past “it raises GH and IGF-1” is extrapolation.
Why is CJC-1295 studied alongside a GHRP or ghrelin mimetic like ipamorelin?
In research and community protocols, CJC-1295 is frequently paired with a growth-hormone-releasing peptide (GHRP) or ghrelin-receptor agonist such as ipamorelin, GHRP-2 or GHRP-6. The rationale is mechanistic and rests on the fact that these two peptide classes act through different receptors and different intracellular pathways on the same somatotroph.
The two-pathway rationale
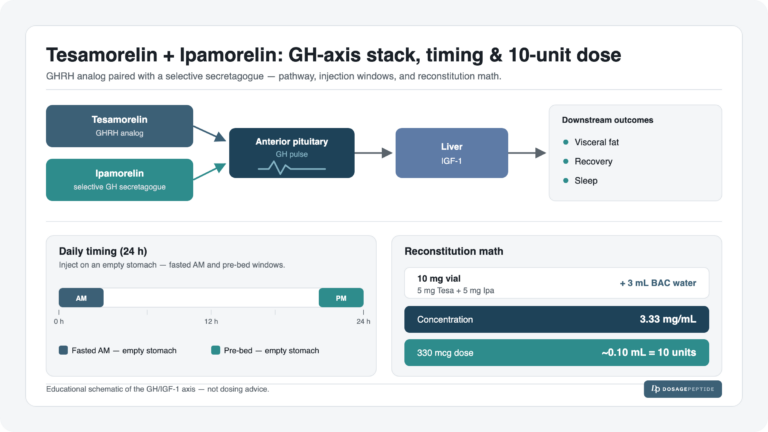
A GHRH analog (like CJC-1295) works through the GHRH receptor and the Gs/cAMP/PKA cascade described above. A GHRP or ghrelin mimetic (like ipamorelin) works through a separate receptor, the growth-hormone-secretagogue receptor GHS-R1a, engaging a phospholipase-C / intracellular-calcium pathway and also acting to reduce somatostatin tone. Because the two inputs converge on the same cell by non-redundant routes, they can potentiate each other. Human endocrine research has shown that co-administering a GHRH analog with a GH-releasing peptide produces markedly synergistic pulsatile GH secretion — a GH response substantially greater than the sum of what either agent produces alone.[4]
There is a third strand to the rationale beyond the two receptors: somatostatin suppression. Ghrelin-receptor agonists do not only add a second stimulatory input; they also appear to reduce somatostatin tone, effectively lifting the brake at the same moment the GHRH analog presses the accelerator. A GHRH analog on its own has to push against whatever somatostatin is present, whereas the pairing pushes harder and pulls back the brake. This three-part logic — two independent stimulatory pathways plus reduced inhibition — is why the combination is described as more than additive.
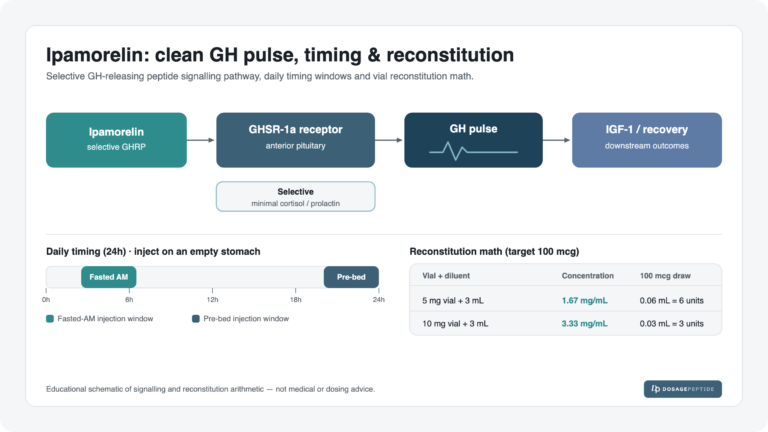
Why is ipamorelin, in particular, so often the chosen partner? Among the GHRPs, ipamorelin is noted for being relatively selective: compared with older secretagogues such as GHRP-6, it is described as having little effect on appetite-driving, cortisol and prolactin release, which is why it is frequently favored in research pairings where a cleaner GH-selective profile is the goal. GHRP-2, another common partner, is a stronger GH releaser but is generally regarded as less selective. The choice of partner therefore shapes the profile of the pairing, not just its raw GH-releasing power.
This is a genuinely well-supported mechanism. What is not well established is a large body of human clinical-outcome trials showing that a CJC-1295 + ipamorelin combination produces specific real-world benefits at defined doses. The synergy is real at the level of GH release physiology; the leap from “more GH release in an assay” to “clinically meaningful outcomes in people” is not something the published human literature has closed. Claims of “5–10x” GH release should be read as mechanistic and preclinical, not as validated human dosing outcomes. For the ipamorelin side specifically, the ipamorelin research protocol guide covers how it is handled in a research context.
For the mechanism-level details of the GHRP side of such pairings, see what ipamorelin is and how it works and the broader guide to how peptides are combined in research. Pre-mixed research blends such as the CJC-1295 no-DAC + ipamorelin blend protocol and the CJC-1295 + GHRP-2 blend protocol exist precisely because of this two-pathway logic.
CJC-1295 vs sermorelin vs tesamorelin: how do the GHRH analogs differ?
CJC-1295 is one of several GHRH-based molecules, and comparing it with sermorelin and tesamorelin clarifies where it sits — and, importantly, which of these are actually approved drugs.
Sermorelin
Sermorelin is simply GHRH(1–29) with no stabilizing substitutions and no albumin handle, so it is very short-acting (half-life on the order of minutes). It was the first GHRH analog to reach the market: the FDA approved it (brand name Geref) for diagnostic use in 1990 and for treating growth-hormone deficiency in children in 1997. The manufacturer voluntarily discontinued it in 2008 as recombinant human GH took over the pediatric market, and the FDA later determined that Geref was not withdrawn from sale for reasons of safety or effectiveness. It remains available through compounding.[6] A dedicated overview is available in what the research says about sermorelin.
Tesamorelin
Tesamorelin is the one clearly FDA-approved molecule in this comparison. It is a synthetic analog based on the full GHRH(1–44) sequence with a trans-3-hexenoic-acid group on the N-terminus that confers DPP-IV resistance. It was approved in 2010 (Egrifta) for reducing excess abdominal visceral fat in HIV-associated lipodystrophy. Its efficacy for that indication was established in large randomized placebo-controlled trials — for example, a 26-week trial in 412 patients reported roughly a 15% reduction in visceral adipose tissue versus an increase on placebo.[7] Tesamorelin therefore shows what a GHRH analog looks like when it has been carried all the way through the clinical-trial and approval process for a defined indication — a bar CJC-1295 has never cleared. More detail is available in the tesamorelin overview.
Where CJC-1295 sits
CJC-1295 occupies a middle ground in chemistry but not in regulatory standing. Its tetrasubstituted backbone makes it more stable than sermorelin, and the DAC form is far longer-acting than any of the others. But unlike tesamorelin, neither CJC-1295 form is an approved drug, and unlike both sermorelin and tesamorelin, it never accumulated a substantial human clinical-trial record. It is best understood as an investigational/research compound with an interesting pharmacology and a thin outcomes literature.
| Molecule | Backbone | Half-life (approx.) | Regulatory status |
|---|---|---|---|
| Sermorelin | Native GHRH(1–29) | Minutes | Previously FDA-approved (Geref); withdrawn 2009, not for safety/efficacy; compounded |
| Tesamorelin | GHRH(1–44) + hexenoyl N-terminus | Short (daily dosing) | FDA-approved (Egrifta) for HIV-associated lipodystrophy |
| CJC-1295 no-DAC (Mod GRF 1-29) | Tetrasubstituted GRF(1–29) | ~30 minutes | Not FDA-approved; research use |
| CJC-1295 with DAC | Tetrasubstituted GRF(1–29) + albumin-binding DAC | ~6–8 days | Not FDA-approved; research use |
Half-life, reconstitution and handling in research settings
Because CJC-1295 is a lyophilized (freeze-dried) peptide, it is reconstituted with a diluent before use in research. General laboratory handling conventions — not human dosing recommendations — include the following:
- Lyophilized peptide is typically stored refrigerated or frozen and protected from light and moisture until reconstitution.
- Reconstitution is commonly performed with bacteriostatic water, added slowly against the vial wall rather than directly onto the peptide pellet, and the vial is swirled rather than vigorously shaken to avoid mechanical stress on the peptide.
- Once reconstituted, the solution is generally kept refrigerated and used within a limited window, as peptides in solution degrade faster than in the dry state.
- Concentration math — converting a vial’s total milligram content and the added diluent volume into a per-unit concentration — is the step most prone to error and should be worked out carefully.
The dramatic half-life difference between the two forms is the single most consequential handling fact: the no-DAC form clears in roughly half an hour, whereas the DAC form remains active for days because it is bound to albumin. That difference has practical implications for how each is studied — a short-acting peptide implies frequent administration to reproduce repeated pulses, while a multi-day peptide implies infrequent administration — and it also means the two forms are not interchangeable on a milligram-for-milligram basis even though they carry the same core sequence.
Why concentration math is the main pitfall
The step most prone to error is not the injection technique but the arithmetic. A vial is labeled by its total peptide content (for example, 2 mg or 5 mg of lyophilized powder), and the concentration of the reconstituted solution depends entirely on how much diluent is added. Add 1 mL of bacteriostatic water to a 5 mg vial and each 0.1 mL contains 500 mcg; add 2 mL to the same vial and that same 0.1 mL now contains only 250 mcg. Nothing about the vial changes — only the diluent volume — yet the per-unit content halves. This is exactly the kind of unit-conversion error that a calculator is meant to eliminate, and it is why documented reconstitution parameters accompany the protocol pages rather than being left to memory.
A few further handling realities are worth stating plainly. Bacteriostatic water (which contains a small amount of benzyl alcohol as a preservative) is generally preferred over sterile water for multi-use vials because it inhibits microbial growth over the days a reconstituted vial is in use. Reconstituted peptide is less stable than the dry powder and degrades faster with heat, light, agitation and freeze-thaw cycling, so it is kept cold and used within a limited window. And because peptides adsorb to surfaces and are damaged by rough handling, the diluent is added gently down the vial wall and the vial is swirled rather than shaken.
The dramatic half-life difference remains the headline. For step-by-step reconstitution technique see the peptide reconstitution guide, and for the concentration arithmetic the reconstitution and dosage calculator. These tools are provided for research accuracy and education, not as clinical instructions. Protocol-specific reconstitution figures appear on the CJC-1295 DAC 2 mg protocol page.
What safety signals and limitations does the literature discuss?
Any honest treatment of CJC-1295 has to foreground how limited the safety data are and how much of what is “known” is extrapolated from the GHRH-analog class or from GH physiology in general rather than from CJC-1295 trials specifically. The single controlled human study reported that the DAC form was relatively well tolerated over its short duration, but “well tolerated in a short Phase 1 study” is a narrow statement that says nothing about repeated or long-term exposure.[1]
Class-level and mechanism-based considerations
- Fluid retention and related effects. Stimulating the GH axis can raise IGF-1 and cause fluid retention, joint discomfort, and tingling/paresthesia — effects well documented for GH and GH-axis stimulation broadly. These are mechanism-based expectations rather than CJC-1295-specific trial findings.
- Injection-site reactions. As with any subcutaneously injected peptide, local reactions (redness, itching, transient swelling) are possible.
- IGF-1 considerations. Sustained elevation of IGF-1 is a theoretical concern in the context of any pro-proliferative signaling. IGF-1 is a growth factor, and while the self-limiting somatostatin feedback discussed earlier caps how high a GHRH analog can push it, the DAC form’s design deliberately keeps IGF-1 elevated for days at a time. That “always-on” pharmacology warrants caution and further study rather than an assumption of safety, particularly over long durations that have never been studied in humans.
- Glucose and insulin sensitivity. Growth hormone is counter-regulatory to insulin, so meaningful, sustained GH elevation can in principle affect glucose handling and insulin sensitivity. This is a recognized effect of the GH axis generally and a reason sustained GHRH-analog signaling is not automatically benign.
- Loss of pulsatility. The DAC form’s continuous GHRH signaling departs from the pulsatile pattern of natural GH secretion, and the long-term consequences of overriding that physiology in humans are simply not characterized.
The DAC formulation’s clinical development history
It is telling that CJC-1295 with DAC never advanced to become an approved product despite being tested in humans in the mid-2000s. The developer’s GHRH-analog program did not carry the DAC molecule through to marketing, and no manufacturer has since brought it to approval for any indication. In assessing peptides used in compounding, the FDA has specifically flagged concerns for substances of this type — including immunogenicity (the potential for injected peptides to provoke an immune response) and impurity-related risks — and CJC-1295 and its DAC variants were among the peptides pulled into that regulatory review process.[8] The absence of an approved product is not, by itself, proof of harm — sermorelin was withdrawn for commercial rather than safety reasons — but it does mean that the extensive post-approval safety monitoring that accompanies a marketed drug simply does not exist for CJC-1295.
Regulatory and product-quality caveats
CJC-1295 in both forms is not an FDA-approved drug for human therapeutic use. In the United States it has also been caught up in the FDA’s review of peptides used in pharmacy compounding: CJC-1295 (and its DAC variants) were among substances handled through the interim 503A “bulks” process and slated for Pharmacy Compounding Advisory Committee review, with the agency citing general concerns about peptides of this type including impurity and immunogenicity risks.[8] The FDA maintains guidance on bulk drug substances in compounding that may present significant safety risks, and the broader regulatory posture toward research peptides continues to evolve.[9]
A practical, non-trivial consequence: material sold for research is not manufactured to pharmaceutical standards. Purity, correct identity, endotoxin levels and actual peptide content can vary between suppliers, and analytical documentation (such as HPLC and mass-spec certificates of analysis) is the only meaningful check — another reason CJC-1295 belongs in the research/investigational category rather than the therapeutic one.
What do we still not know about CJC-1295?
The research gaps are substantial and should temper any confident-sounding claims:
- No clinical-outcome trials. There is no robust human evidence tying CJC-1295 (either form) to outcomes like body composition change, athletic performance, recovery, tissue repair, sleep, or anti-aging endpoints. The human data essentially stop at “it raises GH and IGF-1 for a while.”
- Almost no dedicated human data on the no-DAC form. The best-known human PK/PD study is on the DAC form; the short-acting Mod GRF(1–29) is largely characterized by inference.
- Long-term safety is uncharacterized. Available human data are short-term. The consequences of months or years of sustained IGF-1 elevation, or of continuous non-pulsatile GHRH signaling, are not established.
- The combination-with-GHRP evidence is mechanistic. The synergy with ghrelin mimetics is well supported physiologically but not validated by large human outcome trials at defined doses.
- Optimal use parameters are unknown. Because there are no dose-finding outcome trials, statements about “ideal” frequency or dose are extrapolations, not conclusions.
The responsible summary is that CJC-1295 has a well-understood mechanism and one solid demonstration of prolonged GH/IGF-1 stimulation in humans, sitting atop a large void where clinical-benefit and long-term-safety evidence would normally be.
Frequently Asked Questions
Is CJC-1295 FDA-approved?
No. Neither CJC-1295 with DAC nor CJC-1295 no-DAC (Mod GRF 1-29) is FDA-approved for human therapeutic use. It is handled as a research compound. It has also figured in FDA reviews of peptides used in pharmacy compounding, where the agency raised general concerns about impurities and immunogenicity for peptides of this class. Only tesamorelin (Egrifta), a different GHRH analog, holds FDA approval among GHRH-based molecules.
What is the difference between CJC-1295 with DAC and without DAC?
Both share the same tetrasubstituted GHRH(1–29) backbone. The “with DAC” version adds an albumin-binding appendage that tethers the peptide to serum albumin after injection, extending its half-life to roughly 6–8 days and producing a sustained GH elevation. The “no-DAC” form (Mod GRF 1-29) lacks that appendage, clears in about 30 minutes, and produces a short, more pulse-like GH release.
What is the half-life of CJC-1295?
It depends entirely on the form. CJC-1295 no-DAC has a half-life of roughly 30 minutes. CJC-1295 with DAC has a half-life on the order of 6–8 days because it binds covalently to albumin, a long-lived plasma protein. This roughly hundred-fold difference is the defining distinction between the two products despite their shared backbone.
What does the human research on CJC-1295 actually show?
The main human study (Teichman et al., 2006) tested the DAC form in healthy adults and found that a single subcutaneous dose raised GH about 2- to 10-fold and IGF-1 about 1.5- to 3-fold, with IGF-1 staying elevated for roughly 9–11 days. It was a short-term pharmacodynamic study measuring hormone levels — not clinical outcomes like body composition or performance, which remain unstudied in humans.
Why is CJC-1295 combined with ipamorelin?
CJC-1295 (a GHRH analog) and ipamorelin (a ghrelin-receptor/GHRP agonist) act on different receptors and different intracellular pathways in the same pituitary cells, so they can potentiate each other’s GH-releasing effect. This synergy is well supported at the mechanistic level in cell and endocrine research, but it has not been validated by large human clinical-outcome trials, so combination claims should be read as mechanism-based.
How does CJC-1295 differ from sermorelin and tesamorelin?
All three engage the GHRH receptor. Sermorelin is unmodified GHRH(1–29) and very short-acting; it was FDA-approved (Geref) but discontinued in 2008. Tesamorelin is a modified GHRH(1–44) that is FDA-approved for HIV-associated lipodystrophy with substantial trial support. CJC-1295 is more chemically stabilized than sermorelin and, in DAC form, much longer-acting than either — but it is not an approved drug and has far less human data.
Is CJC-1295 safe?
Its safety is not well characterized. The one key human study reported it was relatively well tolerated over the short term, but there are no long-term human safety data. Mechanism-based concerns include fluid retention, joint discomfort, injection-site reactions, and the theoretical implications of sustained IGF-1 elevation and continuous, non-pulsatile GHRH signaling. Research-grade material also carries purity and identity uncertainties.
What does “DAC” stand for in CJC-1295?
DAC stands for Drug Affinity Complex, a technology from ConjuChem. It refers to a maleimide-bearing chemical appendage on the peptide that, after injection, forms a covalent bond with the free cysteine-34 thiol on serum albumin. By fusing the peptide to long-lived albumin, the DAC dramatically extends the peptide’s half-life from minutes to days.
References
- Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799–805. https://pubmed.ncbi.nlm.nih.gov/16352683/
- Alba M, Fintini D, Sagazio A, et al. Once-daily administration of CJC-1295, a long-acting growth hormone-releasing hormone (GHRH) analog, normalizes growth in the GHRH knockout mouse. Am J Physiol Endocrinol Metab. 2006;291(6):E1290–E1294. https://journals.physiology.org/doi/full/10.1152/ajpendo.00201.2006
- Halmos G, Szabo Z, Dobos N, Juhasz E, Schally AV. Growth hormone-releasing hormone receptor (GHRH-R) and its signaling. Rev Endocr Metab Disord. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12137518/
- Veldhuis JD, Bowers CY. Determinants of GH-releasing hormone and GH-releasing peptide synergy in men. Am J Physiol Endocrinol Metab. 2009;296(5):E1085–E1092. https://pmc.ncbi.nlm.nih.gov/articles/PMC2681313/
- Jetté L, Léger R, Thibaudeau K, et al. Human growth hormone-releasing factor (hGRF)1–29-albumin bioconjugates activate the GRF receptor on the anterior pituitary in rats: identification of CJC-1295 as a long-lasting GRF analog. Endocrinology. 2005;146(7):3052–3058. https://academic.oup.com/endo/article/146/7/3052/2500187
- U.S. Food and Drug Administration. Determination That GEREF (Sermorelin Acetate) Injection Was Not Withdrawn From Sale for Reasons of Safety or Effectiveness. Federal Register. 2013. https://www.federalregister.gov/documents/2013/03/04/2013-04827/determination-that-geref-sermorelin-acetate-injection-05-milligrams-basevial-and-10-milligrams
- Falutz J, Allas S, Blot K, et al. Metabolic effects of a growth hormone-releasing factor (tesamorelin) in patients with HIV. N Engl J Med. 2007;357(23):2359–2370. https://www.nejm.org/doi/full/10.1056/NEJMoa072375
- U.S. Food and Drug Administration. Pharmacy Compounding Advisory Committee; Notice of Meeting; Bulk Drug Substances Nominated for Inclusion on the Section 503A Bulk Drug Substances List. Federal Register. 2024. https://www.federalregister.gov/documents/2024/10/25/2024-24828/pharmacy-compounding-advisory-committee-notice-of-meeting-establishment-of-a-public-docket-request
- U.S. Food and Drug Administration. Certain Bulk Drug Substances for Use in Compounding That May Present Significant Safety Risks. FDA.gov. https://www.fda.gov/drugs/human-drug-compounding/certain-bulk-drug-substances-use-compounding-may-present-significant-safety-risks
- Bongers J, Lambros T, Ahmad M, Heimer EP. Kinetics of dipeptidyl peptidase IV proteolysis of growth hormone-releasing factor and analogs. Biochim Biophys Acta. 1992;1122(2):147–153. https://pubmed.ncbi.nlm.nih.gov/1353684/
- Bermann M, Jaffe CA, Tsai W, DeMott-Friberg R, Barkan AL. Negative feedback regulation of pulsatile growth hormone secretion by insulin-like growth factor I: involvement of hypothalamic somatostatin. J Clin Invest. 1994;94(1):138–145. https://pmc.ncbi.nlm.nih.gov/articles/PMC296291/