Stacking peptides is the practice of running two or more compounds together so their effects overlap rather than compete. Done thoughtfully, a stack lets a research protocol address several rate-limiting steps of the same goal at once — for example pairing a growth-hormone-releasing hormone (GHRH) analog with a selective secretagogue so the two arms of the GH axis reinforce each other, or combining a cytoprotective peptide with a systemic-repair peptide so a recovery model covers both local tissue and whole-body signaling. Done carelessly, a stack simply adds cost, injections and unknowns without adding benefit.
This guide teaches a bottleneck-based framework: instead of asking “which peptides can I pile together,” you ask “what single step is limiting the outcome I am modeling, and which compound is documented to act on that step?” That reframing keeps a stack lean, logical and easier to reason about. We then cover the most common documented research stacks, the timing and separation rules that govern them, and the co-injection question everyone asks — can you combine peptides in one syringe?
One honest sentence on evidence before anything else: the individual compounds discussed here have preclinical literature (and, for a few, human trial data on isolated indications), but peptide stacks as combinations are largely untested in registered human trials. Everything below is presented as the documented research protocol for handling and combining these compounds — it is research-use-only information, not a prescription, dosing recommendation, or medical advice, and none of these combinations is an approved therapy.

At a Glance: Stacking Peptides
| Item | Summary (research-use-only) |
|---|---|
| Core idea | Match each rate-limiting “bottleneck” of a goal to one compound documented to act on it — add compounds only when they cover a different bottleneck. |
| Best-supported synergy | GH axis: a GHRH analog (Tesamorelin, CJC-1295) + a selective secretagogue (Ipamorelin) — two different receptors, one amplified GH pulse. |
| Most common recovery stack | BPC-157 + TB-500 (“Wolverine”): local cytoprotection + systemic cell migration. |
| Timing principle | GH-axis compounds on an empty stomach (pre-bed and/or fasted AM); keep GLP-1 metabolic agents on their own weekly schedule. |
| Same-syringe rule | Only combine compounds reconstituted in compatible diluents with no known pH/stability conflict; keep NAD+ and any acidic-diluent compound separate. Pre-made blends are formulated for you. |
| Number of compounds | Start with one bottleneck. Add a second only when the first is well-tolerated in the research setting. More compounds = more variables. |
| Evidence status | Individual compounds: preclinical to limited human data. Combinations: largely untested in registered human trials. Not FDA-approved as stacks. |
| Exact per-user numbers | Use the interactive dosage calculator; follow the published protocol for each compound in a stack. |
The Bottleneck Framework: Why Stack at All?
Most goals people model with peptides are not limited by a single missing signal — they are limited by a chain of steps, and the slowest step in that chain sets the ceiling. Engineers call that step the bottleneck. Add capacity anywhere except the bottleneck and nothing gets faster; relieve the bottleneck and the whole chain speeds up until a new bottleneck appears. Peptide stacking works the same way.
Take a soft-tissue recovery model. The chain includes local blood flow to the injured area, cell migration into the wound, control of runaway inflammation, and the quality of the collagen laid down. If blood flow is the limiter, more collagen-signaling does nothing. If inflammation is the limiter, more angiogenesis does nothing. A well-designed stack asks which step is actually holding the outcome back, addresses it, then re-evaluates. That is the opposite of the “more is better” instinct that produces six-compound stacks nobody can interpret.
The practical procedure is three questions:
- What is the goal? Be specific — “faster tendon recovery in a research model” is actionable; “feel better” is not.
- What is the rate-limiting bottleneck? Blood flow, cell migration, inflammation, collagen quality, the GH axis, appetite/metabolic signaling, or something else.
- Which single documented compound acts on that bottleneck? Add it. Then, only if a second, distinct bottleneck remains, add a second compound for that step — not a redundant one.
Mapping Bottlenecks to Compounds
The table below is the heart of the framework. Each row is a bottleneck, the plain-English problem it represents, and the compound most commonly documented to target it in research settings. It is deliberately one-compound-per-bottleneck — that discipline is what keeps a stack coherent.
| Bottleneck | Plain-English problem | Commonly researched compound | Why it fits |
|---|---|---|---|
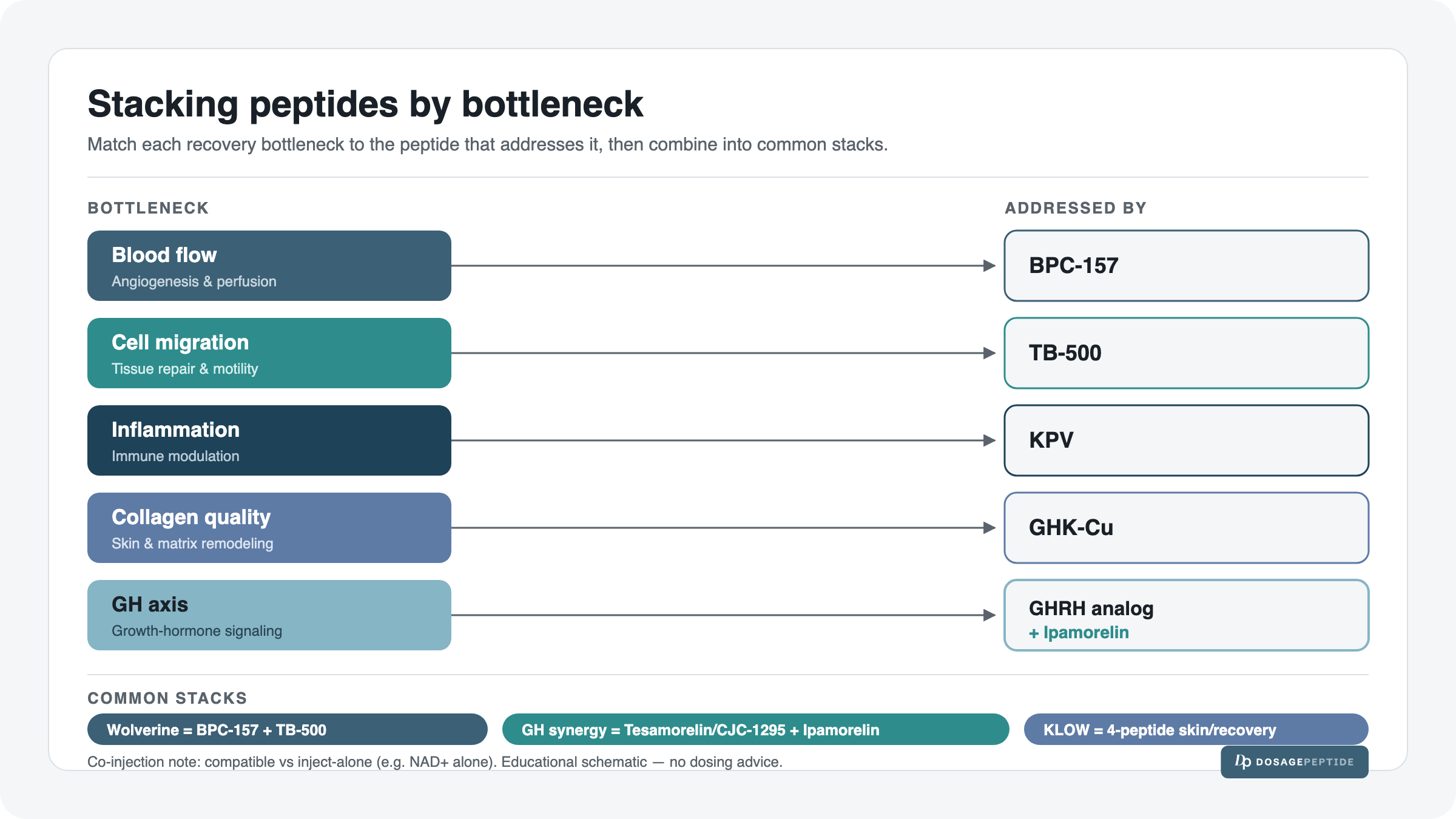
| Blood flow / angiogenesis | Injured tissue is starved of circulation and repair signals. | BPC-157 | Cytoprotective peptide studied for promoting angiogenesis and protecting tissue locally. |
| Cell migration / systemic repair | Repair cells are not reaching the site across the body. | TB-500 (thymosin β4 fragment) | Studied for actin regulation and cell migration — a systemic complement to local action. |
| Runaway inflammation | Chronic gut or tissue inflammation blocks healing. | KPV | Tripeptide fragment studied for anti-inflammatory signaling. |
| Collagen quality / skin & connective tissue | New tissue and skin are structurally poor. | GHK-Cu | Copper peptide studied for remodeling, collagen and skin quality. |
| GH axis (age-related decline) | The natural GH pulse is blunted; recovery and body-composition signaling lag. | GHRH analog + selective secretagogue | Two receptors, one amplified, more physiologic GH pulse (see below). |
| Appetite / metabolic set-point | Energy balance and appetite signaling dominate the outcome. | GLP-1 / dual-agonist agents (Semaglutide, Tirzepatide, Retatrutide) | Incretin-pathway agents studied for appetite and metabolic endpoints — run on their own weekly schedule. |
Notice that many popular “stacks” are simply two adjacent rows of this table — blood flow and cell migration (BPC-157 + TB-500), or the two halves of the GH axis. That is not a coincidence: the durable stacks pair complementary bottlenecks, while the incoherent ones stack two compounds against the same bottleneck and wonder why the second added little.
The GH-Axis Stack: The Best-Supported Synergy
If there is one stack with a clear physiological rationale, it is the GHRH-analog-plus-secretagogue pairing. Growth hormone release from the pituitary is governed by two levers pulling in the same direction through different doors:
- A GHRH analog — such as Tesamorelin or CJC-1295 — binds the GHRH receptor and increases the amplitude of the natural GH pulse.
- A selective secretagogue — Ipamorelin — binds the ghrelin/GHSR-1a receptor and triggers a clean GH pulse with minimal cortisol or prolactin.
Because the two act on distinct receptors, their effect on GH output has been reported as more than additive in research models — one raises the ceiling, the other pulls the trigger, and the combined pulse is larger and more physiologic than either alone. This is why the GH bottleneck row above is the one place the framework deliberately recommends two compounds from the start: a single lever leaves obvious capacity on the table.
Two documented ways to run this synergy:
- As a pre-made blend. The Tesamorelin + Ipamorelin blend protocol combines both compounds in one vial at a documented 10 mg total. This removes any co-injection guesswork — the ratio and diluent are formulated for you.
- As two separate vials, co-timed. A CJC-1295 + Ipamorelin pairing is drawn from two vials and injected in the same session (see the compatibility section on whether they may share a syringe).
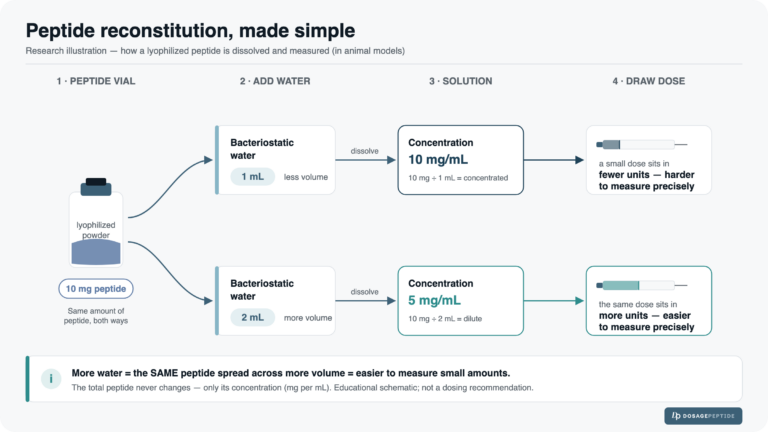
Worked reconstitution: the Tesamorelin + Ipamorelin blend
To show the math is real, here is the full reconstitution arithmetic for the documented blend. The universal formula, taught in depth in our peptide reconstitution guide, is:
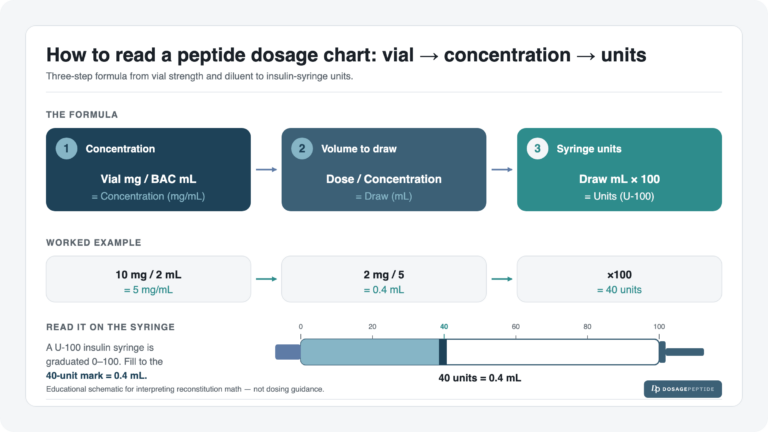
concentration (mg/mL) = vial mg ÷ BAC water mL • draw (mL) = dose ÷ concentration • units on a U-100 syringe = draw mL × 100
For the Tesamorelin + Ipamorelin blend at a documented 10 mg vial reconstituted with 3 mL of bacteriostatic water, at the documented starting dose of 330 mcg (0.33 mg):
| Step | Calculation | Result |
|---|---|---|
| 1. Concentration | 10 mg ÷ 3 mL | 3.33 mg/mL |
| 2. Draw volume | 0.33 mg ÷ 3.33 mg/mL | ≈ 0.10 mL |
| 3. Syringe units (U-100) | 0.10 mL × 100 | ≈ 10 units |
So the documented 330 mcg starting dose of this blend sits at roughly the 10-unit mark on a U-100 insulin syringe. For any other vial size or dose, do not eyeball it — run it through the dosage calculator.
Common Research Stacks
Below are the documented research stacks that recur most often, each mapped back to the bottleneck(s) it relieves. These are documented research protocols, not recommendations, and every one is presented research-use-only.
| Stack | Goal it models | Components | Why they pair (bottlenecks covered) |
|---|---|---|---|
| GH synergy | GH-axis support, recovery, body composition | Tesamorelin + Ipamorelin (or CJC-1295 + Ipamorelin) | GHRH receptor (amplitude) + GHSR-1a (trigger) — two doors, one larger GH pulse. |
| Wolverine (recovery) | Soft-tissue and systemic recovery | BPC-157 + TB-500 | Local cytoprotection/angiogenesis (blood flow) + systemic cell migration. |
| KLOW (skin & recovery blend) | Recovery + skin/connective-tissue quality | KLOW (BPC-157, TB-500, GHK-Cu, KPV, documented 80 mg blend) | Blood flow + cell migration + collagen quality + inflammation — four bottlenecks in one formulated vial. |
| GLOW (skin-forward blend) | Skin quality with recovery support | GLOW blend (documented 70 mg) | Collagen/skin-weighted version of the recovery-plus-skin approach; see the KLOW vs GLOW vs Wolverine comparison. |
| Metabolic + support | Appetite/metabolic set-point, with lean-mass support | A GLP-1/dual-agonist (Semaglutide, Tirzepatide, Retatrutide) run alongside a separate GH-axis or recovery protocol | Metabolic bottleneck handled on its own weekly schedule; GH/recovery compound on its own daily schedule — parallel, not co-injected. |
The three blends — KLOW, GLOW and Wolverine — are worth calling out because they are the cleanest expression of the bottleneck framework: someone has already decided which complementary bottlenecks belong together and formulated a single vial, so you neither co-inject nor guess ratios. If you are choosing between them, the KLOW vs GLOW vs Wolverine breakdown maps each blend to the goal it best fits.
Worked math: the recovery and skin stacks
Three more reconstitution examples, so the numbers behind the most-referenced blended stacks are fully shown. All use a documented 3 mL bacteriostatic-water fill.
| Stack (vial & BAC) | Concentration | Documented starting dose | Draw volume | Units (U-100) |
|---|---|---|---|---|
| KLOW blend — 80 mg / 3 mL | 80 ÷ 3 = 26.67 mg/mL | 2667 mcg (2.667 mg) | 2.667 ÷ 26.67 ≈ 0.10 mL | ≈ 10 units |
| GLOW blend — 70 mg / 3 mL | 70 ÷ 3 = 23.33 mg/mL | 2330 mcg (2.33 mg) | 2.33 ÷ 23.33 ≈ 0.10 mL | ≈ 10 units |
| BPC-157 + TB-500 blend — 10 mg / 3 mL | 10 ÷ 3 = 3.33 mg/mL | 600 mcg (0.6 mg) | 0.6 ÷ 3.33 ≈ 0.18 mL | ≈ 18 units |
All three land at clean, drawable marks on a U-100 syringe. If reading those unit marks is unfamiliar, the insulin syringe units guide walks through exactly where 10 and 18 units sit on the barrel. Note that the two 10-mg blends and the 80-mg KLOW blend land at similar unit marks only because their documented doses were scaled to the vial strength — the same microgram figure would read very differently across them, which is why every stack is computed on its own.
Timing & Separation: Running a Stack Through the Week
A stack is not just which compounds — it is when each one is given. Two principles govern timing.
Principle 1: Respect each compound’s own window
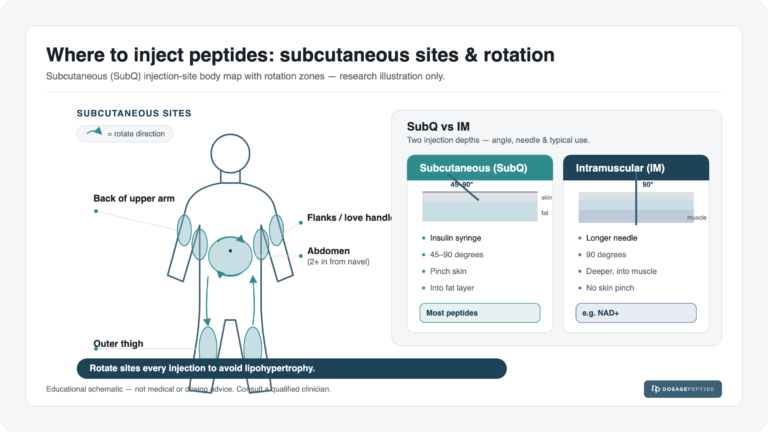
GH-axis compounds are the strictest. GH secretion is blunted by food and by the insulin response to food, so the documented practice is to give GHRH analogs and secretagogues on an empty stomach — a fasted morning dose and/or a pre-bed dose, at least a couple of hours after eating. Pre-bed dosing also stacks the induced pulse onto the body’s largest natural nocturnal GH pulse. GLP-1 and dual-agonist metabolic agents, by contrast, are dosed on a weekly cadence with a gradual titration and are not tied to a fasted window in the same way; their titration schedules are covered in the Semaglutide titration protocol and Tirzepatide titration protocol (linked here as reference — do not repeat their full numbers inside a stack; follow each protocol).
Principle 2: Run together vs. separate
- Run together (same session): compounds that share a window and a route reinforce each other — e.g. a GHRH analog and Ipamorelin both pre-bed, or the two recovery compounds of a Wolverine approach given in one recovery-focused session.
- Separate by schedule, not by hours: a weekly GLP-1 agent and a daily GH-axis protocol simply run on parallel calendars. There is no need to co-time them; they address different bottlenecks on different clocks.
- Separate deliberately: when the goal is local action — e.g. BPC-157 injected near a specific injury as a research practice — that injection is placed for locality and is not merged with a systemic dose.
A worked weekly picture makes this concrete. The grid below is an illustrative research schedule for a two-track stack — a daily GH-synergy blend (pre-bed) plus a separate weekly metabolic agent — showing how the two calendars coexist without collision. It is an example of structure, not a dosing recommendation.
| Track | Mon | Tue | Wed | Thu | Fri | Sat | Sun |
|---|---|---|---|---|---|---|---|
| GH-synergy blend (pre-bed, empty stomach) | Dose | Dose | Dose | Dose | Dose | Off | Off |
| Weekly metabolic agent (own protocol) | Dose | — | — | — | — | — | — |
| Recovery blend (if included; SubQ) | Dose | Dose | Dose | Dose | Dose | Dose | Dose |
The GH track above uses a 5-on / 2-off pattern (a common way to build in receptor rest); a continuous daily pattern is the alternative. The two off-days are optional structure, not a rule. The metabolic track sits on one fixed weekday. The recovery track, when present, often runs daily through an acute phase. Nothing here collides because each track answers to its own protocol.
Can You Combine Peptides in One Syringe? Co-Injection Compatibility
This is the single most-asked stacking question, and the honest answer is: sometimes, and only when the diluents and stability are compatible. Mixing is a pharmacy question about the liquids, not a wishful one about the goals.
The governing factors are:
- Diluent match. Two compounds each reconstituted with plain bacteriostatic water at compatible concentrations are the straightforward case. When one compound is supplied in a different or acidic diluent, mixing risks precipitation or degradation.
- pH and stability. Peptides are stable only within a pH window. Combining a compound formulated at one pH with another at a very different pH can drop one out of solution — you may see cloudiness or particulates, a sign not to inject.
- Known formulations. Some compounds are simply documented to be handled alone. NAD+ is the canonical example: it is typically reconstituted and given on its own, not merged into a shared syringe with other peptides.
| Scenario | Same syringe? | Reason |
|---|---|---|
| A pre-made blend (KLOW, GLOW, Wolverine, Tesamorelin+Ipamorelin) | Already combined for you | The ratio, diluent and stability were formulated in one vial — no mixing decision to make. |
| Two GH-axis compounds from separate vials in compatible BAC water (e.g. CJC-1295 + Ipamorelin) | Commonly co-drawn in research practice | Compatible diluents and pH; same route and window. |
| NAD+ with anything else | Keep separate | Documented to be handled and injected on its own. |
| Two compounds in different or acidic diluents | Do not mix | pH/stability mismatch risks precipitation or degradation. |
| A weekly GLP-1 agent + a daily peptide | No need to mix | Different schedules and routes — run on parallel calendars, separate injections. |
The safest default for anyone new to stacking is to reach for a formulated blend when one exists, and otherwise keep compounds in separate syringes even when co-timed. Separate draws cost one extra needle and remove an entire category of mixing error. General injectable-compatibility and pH considerations for co-administration are pharmacy fundamentals, not peptide-specific magic — when in doubt, do not mix.
Cycle Coordination Across a Stack
Individual protocols each carry a cycle length; a stack has to reconcile them rather than run every compound on the same clock. Three coordination patterns cover most cases:
- Shared cycle. Compounds addressing the same phase of a goal — the two halves of a GH-synergy blend, or the two recovery compounds of a Wolverine approach — naturally start and pause together because they are one protocol.
- Staggered cycle. A recovery blend run through an acute phase can conclude while a longer GH-axis protocol continues underneath it. The recovery track is the shorter, front-loaded layer.
- Parallel independent cycles. A weekly metabolic agent follows its own titration-and-maintenance arc regardless of what the daily peptide track is doing. They share a calendar, not a cycle.
The practical rule: introduce one track at a time. Start a stack with its primary bottleneck compound, confirm it is well-tolerated in the research setting, then layer the second track. Starting three compounds on the same day makes it impossible to attribute any effect — good or bad — to a specific compound.
Safety, Contraindications & Research-Use-Only Framing
Every compound added to a stack multiplies the variables: more injections, more possible interactions, more that can be misattributed. That alone is the strongest argument for the bottleneck discipline — a lean stack is a safer, more interpretable stack.
- Start simple. One bottleneck, one compound. Add a second only after the first is understood and well-tolerated in the research setting.
- Do not mix uncertain diluents. When compatibility is unknown, use separate syringes. Cloudiness or particulates after mixing means discard, not inject.
- Respect each compound’s own safety profile. GH-axis compounds carry considerations such as water retention and IGF-1 effects; GLP-1 agents have their own gastrointestinal and titration considerations. A stack does not erase any single compound’s cautions — it inherits all of them.
- Sterility and handling. Single-use needles, clean technique, correct storage (see how to store peptides before and after reconstitution — more compounds means more vials to store correctly).
- Evidence gap is real. None of these combinations is an FDA-approved therapy, and peptide stacks are largely untested in registered human trials. Any efficacy claim for a combination rests on the mechanistic rationale of the individual compounds, not on trials of the stack itself.
Everything in this guide is a documented research protocol for combining and handling these compounds. It is research-use-only information and not medical advice, a prescription, or a personal dosing recommendation. For any per-user number, use the dosage calculator and follow the published protocol for each compound; to browse every compound’s documented protocol, see the full peptide dosages catalog.
Frequently Asked Questions
Building a stack
How do you stack peptides the right way? Start from the goal, identify the single rate-limiting bottleneck, and add the one compound documented to act on it. Only add a second compound when it covers a different bottleneck — not the same one. This bottleneck-based framework keeps a stack lean and interpretable rather than piling on redundant compounds.
What is a good peptide stack for recovery? The most-referenced recovery pairing is BPC-157 + TB-500 (often called the “Wolverine” combination): BPC-157 covers the local blood-flow/cytoprotection bottleneck and TB-500 covers systemic cell migration. The BPC-157 + TB-500 protocol documents the blend; broader recovery-plus-skin goals often use the KLOW blend instead.
What is the best GH peptide stack? A GHRH analog plus a selective secretagogue — for example Tesamorelin + Ipamorelin, or CJC-1295 + Ipamorelin. The two act on different receptors (GHRH receptor and GHSR-1a), so together they are studied for producing a larger, more physiologic GH pulse than either alone. It is the best-supported synergy in this guide.
How many peptides can I stack at once? There is no fixed number, but the framework’s discipline is one compound per distinct bottleneck. In practice most coherent research stacks are two or three complementary compounds (or a single formulated blend that already contains several). More than that rapidly becomes impossible to attribute or reason about.
Should I use a pre-made blend or separate vials? A pre-made blend (KLOW, GLOW, Wolverine, Tesamorelin+Ipamorelin) removes all mixing and ratio guesswork — the compatible diluent and proportions are formulated for you. Separate vials give flexibility but require you to manage compatibility and timing yourself. For newcomers, a formulated blend is the simpler, lower-error path.
Timing, mixing & compatibility
Can you combine peptides in one syringe? Sometimes — only when the compounds are reconstituted in compatible diluents with no pH or stability conflict. Two GH-axis peptides in plain bacteriostatic water are commonly co-drawn; compounds in different or acidic diluents should not be mixed, and NAD+ is typically kept on its own. If a mixture turns cloudy or shows particulates, discard it. When unsure, use separate syringes.
Which peptides should never be mixed with others? NAD+ is the canonical “handle alone” compound, and any compound supplied in a different or acidic diluent should not be combined with a plain-BAC-water peptide because of pH/stability mismatch. The safe default is to keep compounds separate whenever compatibility is not clearly established.
How do I time peptides in a stack? Respect each compound’s own window. GH-axis compounds go on an empty stomach — fasted morning and/or pre-bed — because food and insulin blunt GH. Weekly GLP-1/dual-agonist agents run on their own fixed-day schedule. Compounds sharing a window and route can be given in one session; compounds on different schedules simply run on parallel calendars.
Do I have to inject stacked peptides at the same time? No. Co-timing only matters for compounds that reinforce each other within the same window (like a GH-synergy pair pre-bed). A weekly metabolic agent and a daily peptide have no reason to be co-timed — they run on separate calendars and separate injections.
Why does the same dose show different unit marks across compounds in my stack? Because units depend on concentration, and concentration depends on vial strength and how much bacteriostatic water you added. An 80 mg blend and a 10 mg blend reconstituted in the same 3 mL yield very different mg/mL, so the same microgram dose lands at a different unit mark. Compute each with the formula or the calculator; the syringe-units guide shows how to read the barrel.
Safety & evidence
Is stacking peptides safe? Each additional compound adds injections, possible interactions and interpretive complexity, so the most cautious approach is to start with one bottleneck and add slowly. A stack inherits every single compound’s cautions — it does not average them away. All of this is research-use-only information, not medical advice, and a qualified healthcare professional should be consulted before any health decision.
Is there human trial evidence for peptide stacks? Individual compounds have preclinical (and in a few cases limited human) data, but peptide stacks as combinations are largely untested in registered human trials. The rationale for a stack rests on the mechanisms of its individual compounds, not on a trial of the combination. That gap should be stated plainly.
Are any of these stacks FDA-approved? No. None of the combinations here is an FDA-approved therapy, and they are presented strictly as documented research protocols for handling these compounds — not prescriptions or treatments.
How do I figure out exact doses and units for my specific stack? Use the interactive dosage calculator for each compound’s vial size and dose, and follow the published protocol for every compound in the stack rather than repeating numbers from memory. For the full list of documented per-compound protocols, browse the dosages catalog.
References
- Individual-compound preclinical literature is cited on each linked protocol guide (internal reference).
- General pharmaceutical references on injectable compatibility and pH considerations for co-administration.
- ClinicalTrials.gov — combination peptide stacks are largely untested in registered human trials (evidence-gap note).
Research-use-only. This article is educational information about documented research protocols for combining and handling peptides. It is not medical advice, a prescription, or a personal dosing recommendation, and none of the combinations described is an FDA-approved therapy. Peptide stacks are largely untested in registered human trials. Consult a qualified healthcare professional before making any health decision. For per-user calculations use the dosage calculator and follow each compound’s published protocol.