Few molecules in the peptide field carry as much genuine scientific weight, and as much marketing exaggeration, as PT-141. Known by its generic name bremelanotide, this synthetic cyclic heptapeptide occupies an unusual position: it is one of the very small number of research peptides that has actually completed the full arc from laboratory bench to a formal U.S. Food and Drug Administration (FDA) approval. In 2019 the FDA approved bremelanotide as Vyleesi for a narrowly defined indication in women, and that single fact separates PT-141 from the vast majority of compounds discussed in the peptide-research community, most of which remain entirely investigational.1
Yet the word “revolutionize” in the title of this article deserves immediate scrutiny. PT-141 did introduce something conceptually new to sexual medicine: it acts on the brain rather than on the blood vessels of the genitals, targeting the central pathways that generate desire itself instead of the downstream hydraulics of erection or lubrication. That is a real mechanistic departure from the phosphodiesterase-5 (PDE5) inhibitors such as sildenafil that dominated the field before it.2 Whether that mechanistic novelty translates into a clinical “revolution,” however, is a much more measured story, one defined by modest effect sizes, a demanding tolerability profile, and a large gap between what has been rigorously proven and what is loosely claimed online.
This article examines PT-141 the way an evidence-cautious reader should: tracing its origin from a sunless-tanning experiment, dissecting its melanocortin mechanism, weighing the actual clinical-trial data honestly, comparing it with related compounds, describing how it is studied and handled in research settings, and stating precisely where the science ends and the speculation begins. Throughout, the regulatory reality is kept front and center: bremelanotide is FDA-approved only for acquired, generalized hypoactive sexual desire disorder (HSDD) in premenopausal women. Every other application, including all use in men and all use for erectile dysfunction, is off-label or purely investigational.1,3
What PT-141 Is and Where It Came From
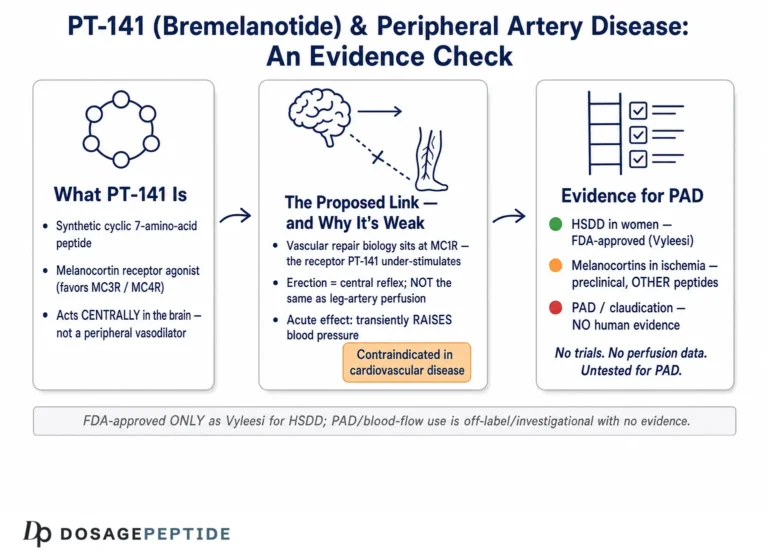
PT-141, or bremelanotide, is a synthetic cyclic seven-amino-acid peptide that functions as a non-selective agonist at melanocortin receptors, with its clinically relevant activity centered on the melanocortin-3 and melanocortin-4 receptor subtypes (MC3R and MC4R).4 Its story is one of the more famous accidents in modern pharmacology. In the 1980s, researchers at the University of Arizona were investigating analogues of alpha-melanocyte-stimulating hormone (alpha-MSH), the natural peptide that darkens skin, as potential agents for sunless tanning and skin-cancer prevention. One of these analogues, Melanotan II, was a superpotent, non-selective melanocortin agonist. During early human self-experimentation with Melanotan II, an unexpected and pronounced effect emerged: spontaneous penile erections and increases in sexual arousal.7
That serendipitous observation redirected an entire line of research. Palatin Technologies acquired the program and set out to design a compound that preserved the sexual-response effects while shedding the properties that made Melanotan II problematic, chiefly its strong activity at the MC1R receptor responsible for skin pigmentation. The result was bremelanotide, which is essentially a metabolite of Melanotan II. Chemically, bremelanotide differs from Melanotan II by having a hydroxyl group where Melanotan II carries a C-terminal amide; this seemingly small change reduces MC1R-driven pigmentation activity while retaining agonism at the receptors that matter for sexual function.5,6 In other words, PT-141 was deliberately engineered from a tanning peptide into a sexual-function peptide.
The early clinical development followed the male erectile-dysfunction route first. Palatin studied both intranasal and, later, subcutaneous formulations in men. But in 2007 the FDA placed the intranasal program on clinical hold because of dose-related increases in blood pressure observed in trial participants.5 This blood-pressure signal became the defining safety concern of the entire bremelanotide story and shaped every subsequent decision about dose, route, and indication. Palatin reformulated the compound as a lower-dose subcutaneous injection and pivoted the primary development target toward female sexual dysfunction, ultimately focusing on hypoactive sexual desire disorder in premenopausal women.
That pivot led, more than a decade later, to the pivotal Phase 3 program and to FDA approval in June 2019 under the brand name Vyleesi, marketed as a 1.75 mg single-use subcutaneous autoinjector.1 It is worth emphasizing the timeline: the molecule that reached pharmacy shelves in 2019 traces directly back to a 1980s tanning experiment, and the approved product represents a highly specific, dose-constrained, narrowly indicated version of a compound that was originally chased for a completely different purpose. The research-community peptide sold as “PT-141,” typically as a lyophilized 10 mg vial, is the same base molecule but is not the FDA-approved finished drug product, is not manufactured to pharmaceutical standards for that use, and carries none of the approved-label protections.
Understanding this origin matters because it explains both the promise and the limits of PT-141. The promise is that it engages a genuine, evolutionarily conserved neuroendocrine system involved in sexual motivation. The limit is that the same broad melanocortin activity that produces the desired central effect also produces nausea, flushing, transient blood-pressure elevation, and skin darkening, all direct consequences of activating melanocortin receptors distributed widely throughout the body. PT-141 is not a precision key for a single lock; it is a broad agonist of an ancient signaling family, and that biology is inseparable from its clinical behavior. Readers seeking the dosing specifics used in the approved product can review the compound-specific PT-141 dosage protocol for the exact label parameters.
How PT-141 Works: The Melanocortin Mechanism
The mechanism of PT-141 is what makes it genuinely distinctive, and it is worth understanding in detail because almost every honest claim about the compound flows from it. Bremelanotide is an agonist at the melanocortin receptor family, a group of five G-protein-coupled receptors (MC1R through MC5R) that respond to melanocortin peptides derived from proopiomelanocortin (POMC). Clinically, bremelanotide’s most important actions are at MC3R and MC4R, which are expressed heavily in the central nervous system, particularly in the hypothalamus and limbic regions that govern appetite, energy balance, and sexual behavior.4
Unlike PDE5 inhibitors, which act peripherally in the corpus cavernosum by preserving cyclic GMP and thereby promoting smooth-muscle relaxation and blood flow, PT-141 works “upstream” in the brain. It is thought to activate MC4R-expressing neurons in the medial preoptic area and related hypothalamic nuclei, structures that integrate sexual motivation and initiate the physiological cascade of arousal.2,4 In the foundational preclinical work published by Molinoff and colleagues in 2003, systemic administration of PT-141 to rats produced penile erections and activated hypothalamic neurons, demonstrated by increased c-Fos immunoreactivity, a standard marker of neuronal activation. The same paper reported that PT-141 induced erections in nonhuman primates and, in early human work, produced rapid, dose-dependent increases in erectile activity in men.4
This is the mechanistic heart of the “revolution” framing: PT-141 does not manufacture an erection or lubrication by force of local vascular action. Instead, it appears to engage the neural circuitry of desire and arousal itself, which is why it can produce effects on subjective sexual interest that a purely vascular drug cannot. The melanocortin system sits at a hub where several pro-sexual neurotransmitter pathways converge, including dopamine and oxytocin signaling. Activation of central melanocortin receptors is believed to modulate this excitatory network, tilting the balance toward sexual motivation.2,4 It is important to state that the precise downstream circuitry in humans is still not fully mapped; the causal chain from MC4R activation to the conscious experience of desire is inferred from animal models, imaging, and pharmacology rather than directly observed in the human brain.
The same central-and-peripheral distribution of melanocortin receptors also explains the compound’s characteristic side effects with mechanistic honesty. Nausea, the single most common adverse event, arises because melanocortin activation influences brainstem centers involved in emesis. Flushing reflects vascular melanocortin effects. Transient increases in blood pressure and decreases in heart rate are a recognized consequence of central and peripheral melanocortin signaling on autonomic tone, which is exactly why the early high-dose intranasal program ran into a blood-pressure hold.5,8 Focal hyperpigmentation, the darkening of patches of skin, gums, or breast tissue, is a direct readout of residual MC1R activity: although bremelanotide was engineered to reduce MC1R stimulation relative to Melanotan II, it does not eliminate it, and repeated dosing can still drive melanin production.1
A crucial nuance is timing and pharmacology. Because PT-141 acts through a receptor-mediated neural mechanism rather than by maintaining a local biochemical state, its effect is not tied to sexual stimulation the way a PDE5 inhibitor’s is. In the approved product, the drug is administered as needed, at least 45 minutes before anticipated sexual activity, with a mean terminal half-life of approximately 2.7 hours.1 The relatively short half-life, combined with rapid subcutaneous absorption (peak plasma concentrations at roughly one hour and near-complete bioavailability), fits its on-demand design. This mechanism-driven pharmacology is fundamental to how researchers model, dose, and interpret the compound, and it is the reason PT-141 is often described as the first centrally acting agent to reach approval in this therapeutic space.
The Clinical Evidence: What the RECONNECT Trials Actually Showed
The evidentiary backbone of PT-141’s approval is a pair of large, well-conducted Phase 3 studies known collectively as the RECONNECT program (trial identifiers including NCT02333071). These were two identically designed, 24-week, randomized, double-blind, placebo-controlled trials that enrolled premenopausal women with acquired, generalized HSDD, with or without decreased arousal, of at least six months’ duration. Participants used a subcutaneous autoinjector to deliver 1.75 mg of bremelanotide on an as-needed basis. The primary results were published by Kingsberg and colleagues in Obstetrics & Gynecology in 2019.3
The trials met their co-primary endpoints. Compared with placebo, bremelanotide produced statistically significant improvements in two validated instruments: the desire domain of the Female Sexual Function Index (FSFI) and the relevant item of the Female Sexual Distress Scale (FSDS) measuring distress associated with low desire. In plain terms, women receiving bremelanotide reported, on average, greater sexual desire and less distress about their low desire than women receiving placebo.3 This is the core positive finding, and it is real: the effect was reproducible across two independent trials, was statistically significant, and was based on validated patient-reported outcomes.
Honesty about the magnitude is essential, however. The effect sizes were modest, and there is a genuine scientific debate about their clinical meaningfulness. The improvements over placebo on the desire and distress scales, while statistically significant, were numerically small, and the placebo response in HSDD trials is characteristically large. A commonly cited real-world anchor is that the change in the number of satisfying sexual events, an outcome many patients care about intuitively, did not differentiate significantly from placebo in these trials. Bremelanotide moved the needle on desire and distress, the constructs it was designed to target, more clearly than on the raw count of satisfying encounters.3 An evidence-cautious reader should hold both facts simultaneously: the drug works better than placebo on its primary measures, and the size of that benefit is small enough that reasonable clinicians differ on how much it matters.
Durability and long-term data come from the open-label extension and the integrated safety analyses. A long-term safety and efficacy analysis reported that improvements were maintained over the extension period and that the safety profile remained consistent, with no new signals emerging over longer exposure.9 A separate integrated analysis of the safety database across the clinical development program, published by Clayton and colleagues in 2022, characterized the adverse-event profile in detail and is discussed further in the safety section below.10 Prespecified subgroup analyses from RECONNECT examined whether particular groups of women, defined by baseline characteristics, responded differently, and generally supported a consistent direction of effect across subgroups.11
Two limitations of even this best-case evidence deserve emphasis. First, the discontinuation rate was notable: a meaningful fraction of participants stopped bremelanotide during the trials, driven substantially by nausea and other tolerability issues. A drug’s benefit is only realized by patients who keep taking it, and the tolerability-driven dropout tempers the practical value of the statistical efficacy.3,10 Second, the entire high-quality evidence base is confined to a single, specific population: premenopausal women with acquired, generalized HSDD. The trials were not designed to, and do not, establish efficacy in postmenopausal women, in women with situational or lifelong low desire, or in men. Extrapolating the RECONNECT results beyond their studied population is not supported by this evidence.
The bottom line on the clinical evidence is therefore nuanced rather than triumphant. PT-141 has a level of human evidence that most research peptides can only dream of: two positive, pre-registered, placebo-controlled Phase 3 trials and an FDA approval built on them. But that evidence supports a modest benefit in a narrow indication, achieved at the cost of a demanding side-effect burden. Calling this a “revolution” is defensible only in the mechanistic sense of being first-in-class; it is not defensible as a claim of large or transformative clinical efficacy.
PT-141 in Men and Other Investigational Uses
Because PT-141’s sexual effects were first discovered in men, and because the compound is widely discussed in male sexual-health circles, it is important to separate the historical research from the current regulatory reality. Bremelanotide is not FDA-approved for any use in men, and it is not approved for erectile dysfunction in anyone. All such use is off-label or investigational.1 That statement is not a technicality; it reflects the fact that the male-ED program was never carried to a successful approval, largely because of the blood-pressure safety signal.
The male research is nonetheless scientifically interesting and forms part of PT-141’s provenance. Early studies evaluated intranasal PT-141 in healthy men and in men with erectile dysfunction, including men who had responded inadequately to sildenafil. A pharmacokinetic and pharmacodynamic study of subcutaneous PT-141 in healthy men and Viagra non-responders documented dose-dependent erectile responses.12 Investigators also explored combining low-dose intranasal PT-141 with sildenafil, reporting an enhanced erectile response with co-administration, an intriguing signal that the central and peripheral mechanisms might be complementary.13 A randomized study by Safarinejad and colleagues reported that bremelanotide, used as a “salvage” therapy in men who had failed sildenafil, produced improvements over placebo; that particular study is, however, the subject of a formal Expression of Concern issued by the Journal of Urology over data-integrity questions, and it should not be treated as reliable evidence.14
These male-ED findings, taken together, established the proof of concept that central melanocortin agonism can influence human erectile function. But proof of concept is not approval. The intranasal program was halted by the FDA in 2007 over dose-related hypertension, and the male subcutaneous program did not ultimately produce an approved product. The reason is instructive: in men, the drug’s efficacy did not clearly outweigh its cardiovascular and tolerability liabilities at the doses required, and effective, well-tolerated PDE5 inhibitors already dominated the market. The competitive and safety landscape, not merely the biology, determined the outcome.5
Beyond sexual function, the melanocortin system’s role in energy balance has driven interest in bremelanotide and related melanocortin agonists for metabolic effects. Because MC4R is a central regulator of appetite and body weight, melanocortin agonism can reduce food intake; two Phase 1 randomized controlled trials of intensive short-term bremelanotide dosing in women with obesity reported statistically significant reductions in caloric intake (on the order of roughly 400 kcal/day) and modest reductions in body weight versus placebo over about two weeks.16 This metabolic dimension is real biology but should be regarded as exploratory for bremelanotide specifically; it is not an approved use, and the more advanced melanocortin work in obesity has centered on other, MC4R-selective agents rather than on PT-141. Framing PT-141 as a “weight-loss peptide” on the basis of these observations would substantially overstate the evidence.
The broader point for readers is a discipline about labels. On the internet, PT-141 is frequently marketed as a unisex libido enhancer, a male ED treatment, and sometimes as a general “wellness” or performance compound. The rigorous human evidence supports exactly one of these framings, and only partially: modest benefit for desire and distress in premenopausal women with a specific diagnosis. Everything else about men, about erectile dysfunction, about postmenopausal women, and about metabolic effects, ranges from genuinely investigational (with real but incomplete data) to purely speculative. An honest reader keeps these tiers distinct rather than collapsing them into a single optimistic story. For a structured comparison of how different sexual-health and recovery peptides are positioned, the site’s broader peptide dosage catalog lays out compound-by-compound protocols and their evidence context.
How PT-141 Compares With PDE5 Inhibitors and Related Compounds
The most illuminating way to understand PT-141’s place in sexual medicine is by contrast. The dominant class of sexual-dysfunction drugs before bremelanotide, and still today, is the PDE5 inhibitor family: sildenafil (Viagra), tadalafil (Cialis), vardenafil, and avanafil. These act peripherally to enhance penile blood flow and require sexual stimulation to work. PT-141 acts centrally on desire and arousal circuitry and, at least in principle, does not require a pre-existing arousal state to initiate its effect. The two classes address different links in the chain of sexual response: PDE5 inhibitors address the plumbing, PT-141 addresses the drive.2,4
This distinction is precisely why PT-141 was pursued for HSDD in women, a condition defined by absent or low desire and the distress it causes, rather than by a mechanical failure of arousal. PDE5 inhibitors have never been convincingly effective for female low desire, because increasing genital blood flow does not create the motivational state that is missing. A centrally acting agent is mechanistically better matched to the problem, which is the genuine conceptual advance PT-141 represents.3
The other FDA-approved drug for premenopausal HSDD, flibanserin (Addyi), offers a useful within-indication comparison. Flibanserin is a daily oral medication that modulates serotonin, dopamine, and norepinephrine signaling; it must be taken every day, carries warnings about hypotension and syncope especially with alcohol, and also delivers modest efficacy. Bremelanotide, by contrast, is an as-needed subcutaneous injection taken before anticipated activity. The trade-offs are clear: flibanserin requires chronic daily dosing and alcohol caution but avoids injections; bremelanotide is on-demand but requires a subcutaneous shot and carries a high rate of nausea. Neither is a large-effect therapy, and the choice between them in clinical practice hinges on tolerability and patient preference rather than on a decisive efficacy advantage.3
Within the peptide world, PT-141 is frequently discussed alongside its ancestor Melanotan II and alongside unrelated recovery peptides. The Melanotan II comparison is the most important to get right. Melanotan II is a non-selective melanocortin agonist with strong MC1R (pigmentation) activity; it is not approved for any indication, is associated with significant safety concerns, and its sexual effects come bundled with pronounced tanning, nausea, and other melanocortin effects. Bremelanotide is the more refined, MC1R-reduced descendant designed specifically to separate the sexual-response effect from the pigmentation effect, and it alone carries an FDA approval.5,6 Conflating the two, as some vendor marketing does, is scientifically inaccurate.
The table below summarizes the principal contrasts. It is intended as an educational comparison of mechanisms and regulatory status, not as clinical guidance.
| Feature | PT-141 (bremelanotide) | PDE5 inhibitors (e.g., sildenafil) | Flibanserin (Addyi) |
|---|---|---|---|
| Primary site of action | Central (brain, MC3R/MC4R) | Peripheral (penile vasculature) | Central (serotonin/dopamine/NE) |
| Target of effect | Sexual desire and arousal | Erectile hydraulics | Sexual desire |
| Dosing pattern | As-needed subcutaneous injection | As-needed oral | Daily oral |
| FDA-approved population | Premenopausal women with acquired, generalized HSDD | Men with erectile dysfunction | Premenopausal women with acquired, generalized HSDD |
| Most common limitation | Nausea; transient blood-pressure rise | Headache, flushing; cardiac/nitrate caution | Hypotension/syncope, alcohol caution; daily dosing |
| Effect size | Modest | Large for ED | Modest |
The comparison reinforces the article’s central theme. PT-141’s claim to significance is not that it works better than existing drugs, it does not outperform PDE5 inhibitors for erectile dysfunction, but that it works on a different and previously underserved target, desire, in a population for whom the vascular drugs were never suited. That is a real but bounded contribution.
Research Models and Study Methodology
Understanding how PT-141 has been studied clarifies why some claims are well-supported and others are not. The evidence for bremelanotide spans the classic translational hierarchy: in vitro receptor pharmacology, animal models, human pharmacokinetic and pharmacodynamic studies, and finally randomized controlled trials. Each tier answers a different question, and each has characteristic limits.4
At the molecular level, in vitro receptor-binding and functional assays established bremelanotide as an agonist across melanocortin receptor subtypes, with the affinity and activation profile that defines its pharmacology. These assays are essential for confirming that the molecule engages MC3R and MC4R, but by design they say nothing about behavior, efficacy, or safety in a living organism. Any claim that rests solely on “it binds MC4R” is a molecular claim, not a clinical one.4
At the animal level, the foundational studies used rodent and nonhuman-primate models to demonstrate that systemic PT-141 produces penile erections and activates specific hypothalamic neuronal populations, indexed by c-Fos expression. In females, preclinical and early translational work used physiological measures of genital response, such as vaginal photoplethysmography, to quantify arousal.4 These models are powerful for establishing mechanism and dose-response relationships, but the leap from a rat’s erectile reflex or a c-Fos signal to a woman’s subjective experience of desire is enormous. Animal models can demonstrate that a compound engages sexual circuitry; they cannot validate a subjective human outcome. This is precisely why regulators require human trials with patient-reported endpoints.
The human pharmacology tier characterized how bremelanotide behaves in the body: near-100% subcutaneous bioavailability, peak concentrations around one hour, a terminal half-life of roughly 2.7 hours, low plasma protein binding (about 21%), and elimination through both renal and fecal routes. These parameters, drawn from the FDA-approved labeling, are what make the on-demand, pre-activity dosing schedule pharmacologically coherent.1 Dedicated cardiovascular studies, including ambulatory blood-pressure monitoring, were conducted specifically to quantify the small but real blood-pressure effects that had triggered the earlier clinical hold.8
The randomized controlled trial tier is the gold standard and, for bremelanotide, is exemplified by the RECONNECT program. The methodological strengths there are substantial: two identically designed trials (replication), randomization, double-blinding, placebo control, pre-specified co-primary endpoints, validated patient-reported instruments (FSFI desire domain and FSDS), and adequate sample sizes and duration to detect a modest effect.3 The use of validated instruments matters enormously in a field where the outcome, sexual desire, is inherently subjective; a poorly validated questionnaire could manufacture significance where none exists. The large placebo response typical of sexual-medicine trials is exactly why placebo control and blinding are non-negotiable, and it is the main reason effect sizes must be interpreted relative to placebo rather than against baseline.
A methodological caution that recurs throughout the PT-141 literature is the distinction between statistical and clinical significance. The RECONNECT trials achieved statistical significance on their co-primary endpoints, but the magnitude of benefit and the failure to significantly move the count of satisfying sexual events illustrate that a statistically significant result can coexist with a debatable clinical impact.3 For any reader evaluating peptide claims, this is the single most transferable lesson: always ask not only “was it significant?” but “how large was the effect, in which population, and measured how?” Applied to PT-141, those questions yield a picture of a genuine, replicated, but modest effect in a narrowly defined group, which is very different from the sweeping claims that circulate in non-scientific sources.
Safety, Tolerability, and Contraindications
PT-141’s safety profile is, in many ways, the decisive factor in its clinical story, and it is well characterized precisely because the compound completed a full FDA development program. The integrated safety analysis by Clayton and colleagues and the approved labeling together provide a detailed and reliable picture.1,10 The dominant theme is that bremelanotide’s tolerability, not any catastrophic toxicity, is what constrains its use.
The most common adverse event by a wide margin is nausea. Across the pivotal trials, nausea occurred in roughly 40% of women receiving bremelanotide versus a very low rate on placebo. It typically begins within about an hour of dosing, lasts approximately two hours, is most pronounced after the first dose, and often lessens with subsequent doses; nonetheless, a meaningful number of participants used anti-nausea medication or discontinued because of it.1,3 Flushing (about 20%) and headache (about 11%) are the next most frequent, with injection-site reactions also reported.1 These rates are high enough that tolerability, rather than efficacy, is often the deciding factor in whether the drug is continued.
Two safety issues warrant particular emphasis because they define the boundaries of appropriate use. The first is cardiovascular. Bremelanotide causes small, transient increases in blood pressure and reductions in heart rate after each dose, a direct consequence of melanocortin activity on autonomic tone. Ambulatory blood-pressure monitoring confirmed these effects are modest at the approved dose but real.8 Consequently, the label contraindicates bremelanotide in people with uncontrolled hypertension or known cardiovascular disease, and this same signal is what ended the higher-dose intranasal program historically.1,5 This is not a theoretical concern; it is the central reason the compound is dose-limited and route-limited.
The second is focal hyperpigmentation: darkening of patches of skin, and also of the gums and breast tissue, reflecting residual MC1R (pigmentation) activity. This was rare when the drug was used within the labeled limits but occurred in more than a third of subjects when dosed daily for extended periods in earlier studies, which is why daily use is explicitly discouraged. Critically, the hyperpigmentation did not always resolve after discontinuation, and the risk is higher in individuals with darker skin. The label advises considering discontinuation if it develops.1 This adverse effect is a direct illustration of why dosing frequency limits exist and why “more is better” reasoning is dangerous with this compound.
There is also a clinically important drug interaction: bremelanotide slows gastric emptying and can significantly reduce the absorption and systemic exposure of orally administered drugs. The label specifically warns against use with oral naltrexone-containing products used to treat alcohol or opioid dependence, because reduced naltrexone exposure could cause treatment failure with serious consequences.1 This interaction is a reminder that PT-141’s pharmacology reaches well beyond sexual circuitry.
To bound the risk picture honestly in the other direction: no unexpected serious toxicities emerged over the longer-term open-label exposure, and the overall profile was characterized by the developers and regulators as manageable within the labeled constraints.9,10 Post-marketing pharmacovigilance has separately described a single reported case of clinically apparent liver injury attributed to bremelanotide, which independent drug-injury monitoring classifies as a possible but uncommon and low-likelihood cause of drug-induced liver injury rather than an established hepatotoxin.15 The safety story is therefore not one of danger so much as one of demanding tolerability plus specific, well-defined contraindications. The following table summarizes the principal safety considerations from the approved labeling; it is educational and does not replace the full prescribing information or professional medical advice.
| Safety domain | Key findings (approved product) |
|---|---|
| Most common adverse events | Nausea (~40%), flushing (~20%), headache (~11%), injection-site reactions |
| Cardiovascular | Transient rise in blood pressure, fall in heart rate; contraindicated in uncontrolled hypertension or known cardiovascular disease |
| Skin/pigmentation | Focal hyperpigmentation (skin, gums, breast); higher with frequent dosing and darker skin; may not resolve on discontinuation |
| Drug interactions | Slows gastric emptying; avoid with oral naltrexone; may reduce absorption of oral drugs |
| Dosing limits (label) | 1.75 mg subcutaneous, at least 45 minutes before activity; no more than one dose per 24 hours; maximum 8 doses per month |
Handling and Reconstitution in a Research Context
It is essential to draw a sharp line here. The FDA-approved product, Vyleesi, is supplied as a pre-filled, single-use subcutaneous autoinjector containing 1.75 mg of bremelanotide; it requires no reconstitution and is used exactly as the prescribing information directs.1 The material typically encountered in the research-peptide market, by contrast, is a lyophilized (freeze-dried) powder, commonly labeled as a 10 mg vial, sold strictly for laboratory research and explicitly not for human use. Discussing handling and reconstitution of that research material is a matter of laboratory technique and accuracy, not a set of instructions for self-administration, and nothing in this section should be read as endorsing human use of non-approved product.
In a research setting, lyophilized peptides are reconstituted with a suitable diluent, most commonly bacteriostatic water (sterile water containing 0.9% benzyl alcohol), which allows multiple withdrawals from a vial over a limited period. The core of accurate handling is straightforward arithmetic: the final concentration equals the mass of peptide in the vial divided by the volume of diluent added. For a 10 mg vial reconstituted with 3.0 mL of diluent, the resulting concentration is approximately 3.33 mg/mL, meaning each 0.1 mL contains about 0.333 mg (333 mcg). Choosing the diluent volume is therefore a way of setting the concentration to a range that makes the intended measured amounts fall within convenient, readable syringe markings.
Precision matters because the difference between milligrams and micrograms is a factor of one thousand, and misreading an insulin-syringe scale is the most common source of catastrophic dosing error in any peptide context. Insulin syringes are graduated in “units,” where 100 units equals 1.0 mL; translating a target mass into units requires knowing the reconstituted concentration and doing the conversion deliberately rather than by habit. Researchers routinely use a written calculation, and increasingly a validated tool, to avoid slip errors. The site’s peptide reconstitution calculator automates the concentration-to-volume math, and the accompanying step-by-step reconstitution guide walks through diluent selection, mixing technique, and syringe reading in detail.
Handling technique protects both accuracy and stability. Bacteriostatic water is added slowly, directed against the vial wall rather than blasted onto the powder, and the vial is swirled gently rather than shaken, because peptides are fragile molecules whose higher-order structure can be disrupted by mechanical shear and foaming. The powder should be allowed to dissolve fully into a clear solution; cloudiness or persistent particulates indicate a problem. From a research-integrity standpoint, documenting the lot, the diluent, the reconstitution date, and the resulting concentration is standard practice, because a solution of unknown provenance is a solution of unknown concentration.
Stability and storage are equally important. Lyophilized peptide is generally stored frozen or refrigerated and kept away from light and moisture; once reconstituted, the solution is refrigerated and used within a limited window, with bacteriostatic water offering some protection against microbial growth compared with plain sterile water. Repeated freeze-thaw cycles of the reconstituted solution are avoided because they degrade peptide integrity. These are generic good-laboratory-practice principles rather than PT-141-specific magic, but they determine whether the concentration a researcher calculated on paper is actually the concentration in the vial weeks later. These are general good-laboratory-practice principles that apply to peptide handling broadly rather than claims specific to any one vendor’s product.
The overarching point is one of quality and honesty. Research-grade peptide is not manufactured, tested, or labeled to the standard of an approved drug; purity, actual peptide content, and sterility can vary between sources, and a vial labeled “10 mg” is only as trustworthy as its supplier’s analytics. This uncertainty is one more reason the approved product exists as a fixed-dose autoinjector: it removes reconstitution error and content variability from the equation entirely. For the exact label-derived parameters and titration ranges discussed in research contexts, the dedicated PT-141 protocol page consolidates the numbers in one place.
Limitations and the Human-Evidence Gap
Having surveyed what PT-141 does and where the data come from, it is worth stating plainly what remains unknown or unproven, because the gap between the approved reality and the online mythology is where readers are most often misled. PT-141 sits in an unusual middle ground: it has far more human evidence than a typical research peptide, yet that evidence is narrow enough that most of the ways the compound is actually used and discussed are unsupported by it.1,3
The first and largest gap concerns population. Every claim with strong human support applies to premenopausal women with acquired, generalized HSDD. There are no comparable Phase 3 data establishing efficacy in postmenopausal women, in women whose low desire is lifelong or situational rather than acquired and generalized, or in men for any indication. The male-ED studies, while real, are older, smaller, and were never carried to approval; the metabolic observations are exploratory. Using RECONNECT to justify use in any of these other groups is an extrapolation the data do not license.3,12
The second gap concerns effect size and durability of clinical meaning. As discussed, the benefit over placebo, while statistically robust and replicated, is modest, and the failure to significantly increase the count of satisfying sexual events invites honest debate about how much the drug changes lived experience. Long-term data extend to the open-label follow-up but do not answer questions about effects over many years of intermittent use, and the high tolerability-driven discontinuation rate means real-world persistence, and therefore real-world benefit, may be lower than trial efficacy suggests.3,9
A third gap is mechanistic precision in humans. The melanocortin-to-desire causal chain is well supported in animals and pharmacologically plausible in people, but the specific human neural circuitry, the individual variability in response, and the reasons some people respond and others do not are not fully understood. This matters because it means there is currently no way to predict responders, and the “desire” endpoint itself is subjective and context-dependent in ways that resist reduction to a single receptor mechanism.2,4
A fourth and critical gap, specific to the research-peptide market, is product identity and quality. The rigorous evidence pertains to a pharmaceutical-grade, fixed-dose autoinjector manufactured and tested to approval standards. It does not transfer automatically to a lyophilized vial from a research supplier, which may differ in purity, actual content, sterility, and stability. Efficacy and safety data generated with the approved product cannot be assumed to describe the behavior of a chemically similar but differently manufactured and differently dosed material.1
Finally, there is the general limitation that governs all of peptide science: the ubiquity of overstatement. Vendor pages, testimonials, and social media routinely present PT-141 as a broadly effective libido enhancer for anyone, frequently citing the FDA approval as if it validated all uses. It does not. The approval is a narrow, specific, hard-won result for one indication in one population, achieved despite a demanding side-effect profile. An evidence-cautious reader treats the FDA approval as strong evidence for exactly what it covers and as no evidence at all for the many uses it does not. Holding that line is the difference between using the science and being used by the marketing. For a wider view of how sexual-health and recovery peptides are stacked and combined in research discussions, the peptide stacks reference catalogs common combinations alongside their evidentiary caveats.
Regulatory Status Around the World
The regulatory status of bremelanotide is the anchor for every honest statement about the compound, so it deserves a precise summary rather than a vague gesture at “FDA-approved.” In the United States, the FDA approved bremelanotide as Vyleesi in June 2019, indicated specifically for the treatment of acquired, generalized hypoactive sexual desire disorder (HSDD) in premenopausal women, characterized by low sexual desire that causes marked distress or interpersonal difficulty and is not due to a co-existing medical or psychiatric condition, problems within the relationship, or the effects of a medication or other drug substance.1
Each qualifier in that indication is load-bearing. “Acquired” means the low desire developed after a period of normal function, excluding lifelong low desire. “Generalized” means it occurs across situations and partners, excluding situational low desire tied to a specific context. “Premenopausal” excludes postmenopausal women, in whom efficacy was not established. And the exclusion of desire problems attributable to other medical, psychiatric, relationship, or drug causes reflects that HSDD is a diagnosis of a specific disorder, not a label for any low libido. The approval is therefore far narrower than the phrase “approved for low sex drive” implies.1,3
Equally important is what the FDA did not approve. Bremelanotide is not approved for erectile dysfunction, not approved for any use in men, and not approved for postmenopausal women. It is not approved for weight loss, energy, athletic performance, or general “wellness.” Any use outside the labeled indication is off-label (if prescribed by a clinician using the approved product) or investigational, and any use of research-grade PT-141 powder is outside the approved regulatory framework entirely, since that material is sold for laboratory research and not as a drug for human administration.1
Internationally, bremelanotide’s footprint is far more limited than its U.S. approval and online prominence might suggest. It has not achieved the broad global approvals that many blockbuster drugs enjoy; regulatory availability varies by jurisdiction, and in many countries the compound is not authorized for marketing at all. Readers outside the United States should not assume that U.S. approval implies availability or legality in their own country, and the specific legal status of possessing or using research-grade peptide differs substantially between jurisdictions. The compound’s earlier history, including the 2007 FDA clinical hold on the intranasal formulation over blood-pressure concerns, is part of why its regulatory path was long and its final approval narrow.5
The regulatory bottom line frames the entire “revolutionize” question honestly. PT-141 genuinely earned a place in the regulatory record as a first-in-class, centrally acting agent for a real and previously underserved condition, an achievement no other peptide in the sexual-health space can currently claim. But that achievement is defined by its boundaries: one indication, one population, one dose regimen, and a set of contraindications and warnings that reflect a demanding safety profile. The scientifically accurate reading is that PT-141 opened a new mechanistic door in sexual medicine while delivering a modest, tightly bounded clinical benefit, which is a meaningful contribution but not the sweeping transformation that the word “revolutionize” colloquially suggests.1,3
Frequently Asked Questions
Is PT-141 (bremelanotide) FDA-approved?
Yes, but narrowly. The FDA approved bremelanotide as Vyleesi in 2019 for acquired, generalized hypoactive sexual desire disorder (HSDD) in premenopausal women, delivered as a 1.75 mg single-use subcutaneous autoinjector.1 It is not approved for erectile dysfunction, for any use in men, or for postmenopausal women. All of those applications are off-label or investigational, and research-grade PT-141 powder is sold for laboratory use only, outside the approved-drug framework.1
How is PT-141 different from Viagra (sildenafil)?
They act on different links in the sexual-response chain. PDE5 inhibitors like sildenafil act peripherally to enhance genital blood flow and require sexual stimulation to work; they address the mechanics of erection. PT-141 acts centrally in the brain on melanocortin (MC3R/MC4R) circuitry involved in sexual desire and arousal.2,4 This is why PT-141 was developed for low desire in women, a problem the vascular drugs do not address, rather than as a competitor to Viagra for erectile dysfunction.
Does PT-141 work for men or for erectile dysfunction?
There is genuine early research in men, including studies in men who did not respond to sildenafil, showing dose-dependent erectile responses, and this male work is part of the compound’s history.12 However, the male and erectile-dysfunction programs were never carried to FDA approval, in part because of dose-related blood-pressure increases that led to a 2007 clinical hold on the intranasal formulation.5 Any use in men today is off-label or investigational, not an approved indication.
How effective is PT-141, really?
In the two Phase 3 RECONNECT trials, bremelanotide produced statistically significant improvements over placebo in sexual desire and in distress about low desire, and these results replicated across both trials.3 The honest caveat is that the effect sizes were modest, and the drug did not significantly increase the number of satisfying sexual events versus placebo. It is a real, replicated, but small benefit in a specific population, not a large or transformative effect.3
What are the most common side effects?
Nausea is by far the most common, affecting roughly 40% of women in trials; it usually starts within an hour, lasts about two hours, and often lessens with later doses.1,3 Flushing (about 20%) and headache (about 11%) are next, along with injection-site reactions. More specific concerns include transient blood-pressure increases (with contraindication in uncontrolled hypertension or known cardiovascular disease) and focal hyperpigmentation, darkening of skin, gums, or breast tissue, which is more likely with frequent dosing and may not fully resolve.1,8
Where does PT-141 come from?
It descends from Melanotan II, a non-selective melanocortin agonist originally studied at the University of Arizona in the 1980s as a sunless-tanning agent, which unexpectedly produced sexual arousal and erections in early testing.7 Bremelanotide is essentially a refined metabolite of Melanotan II, engineered to reduce the skin-pigmentation (MC1R) activity while retaining the sexual-response effects mediated by MC3R and MC4R.5,6
Why does the approved dose have monthly limits?
The label recommends no more than one 1.75 mg dose per 24 hours and no more than eight doses per month.1 These limits exist largely to manage the dose- and frequency-dependent risks: focal hyperpigmentation rose sharply with daily dosing in earlier studies, and blood-pressure effects and nausea are also related to dose and frequency. The frequency cap is a direct, mechanistically motivated safety constraint, not an arbitrary rule.1,5
Is research-grade PT-141 the same as Vyleesi?
No. Vyleesi is a pharmaceutical-grade, fixed-dose autoinjector manufactured and tested to FDA approval standards, requiring no reconstitution.1 Research-grade PT-141 is typically a lyophilized powder sold for laboratory use only; its purity, actual peptide content, sterility, and stability can vary by supplier, and it must be reconstituted and measured manually, introducing error the approved product eliminates. The clinical evidence generated with the approved product does not automatically describe the behavior of a differently manufactured research material.
Closing Note
This article is provided for educational and research-informational purposes only. It is not medical advice, and nothing in it should be interpreted as a recommendation to obtain, administer, or use PT-141 (bremelanotide) or any other compound. PT-141 is FDA-approved only as Vyleesi for acquired, generalized hypoactive sexual desire disorder in premenopausal women; all other uses are off-label or investigational, and research-grade peptide is not intended for human use. Sexual health, medication decisions, and any question about a compound’s suitability, safety, or legality should be discussed with a qualified, licensed healthcare professional who knows your individual history. Statements about mechanisms, effects, and safety reflect the state of the published evidence at the time of writing and may change as new research emerges.
References
- U.S. Food and Drug Administration. VYLEESI (bremelanotide injection) Full Prescribing Information, 2019. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/210557s000lbl.pdf
- Pfaus J, Giuliano F, Gelez H. Bremelanotide: an overview of preclinical CNS effects on female sexual function. J Sex Med. 2007;4(Suppl 4):269-279. PMID 17958619. https://pubmed.ncbi.nlm.nih.gov/17958619/
- Kingsberg SA, Clayton AH, Portman D, et al. Bremelanotide for the Treatment of Hypoactive Sexual Desire Disorder: Two Randomized Phase 3 Trials. Obstet Gynecol. 2019;134(5):899-908. https://pubmed.ncbi.nlm.nih.gov/31599840/
- Molinoff PB, Shadiack AM, Earle D, Diamond LE, Quon CY. PT-141: a melanocortin agonist for the treatment of sexual dysfunction. Ann N Y Acad Sci. 2003;994:96-102. https://pubmed.ncbi.nlm.nih.gov/12851303/
- Dhillon S, Keam SJ. Bremelanotide: First Approval. Drugs. 2019;79(14):1599-1606. (Peer-reviewed development history, including the intranasal-to-subcutaneous switch driven by blood-pressure increases and the halting of the earlier intranasal program.) https://link.springer.com/article/10.1007/s40265-019-01187-w
- King SH, Mayorov AV, Balse-Srinivasan P, Hruby VJ, Vanderah TW, Wessells H. Melanocortin receptors, melanotropic peptides and penile erection. Curr Top Med Chem. 2007;7(11):1111-1119. PMID 17584130. https://pmc.ncbi.nlm.nih.gov/articles/PMC2694735/
- Dorr RT, Lines R, Levine N, Brooks C, Xiang L, Hruby VJ, Hadley ME. Evaluation of melanotan-II, a superpotent cyclic melanotropic peptide in a pilot phase-I clinical study. Life Sci. 1996;58(20):1777-1784. PMID 8637402. (Primary University of Arizona Melanotan II study documenting spontaneous erections during human dosing.) https://pubmed.ncbi.nlm.nih.gov/8637402/
- Shadiack AM, et al. Usefulness of ambulatory blood pressure monitoring to assess the melanocortin receptor agonist bremelanotide. PMC5338879. https://pmc.ncbi.nlm.nih.gov/articles/PMC5338879/
- Simon JA, Kingsberg SA, Portman D, et al. Long-Term Safety and Efficacy of Bremelanotide for Hypoactive Sexual Desire Disorder. Obstet Gynecol. 2019. PMC6819023. https://pmc.ncbi.nlm.nih.gov/articles/PMC6819023/
- Clayton AH, Kingsberg SA, Portman D, et al. Safety Profile of Bremelanotide Across the Clinical Development Program. J Womens Health (Larchmt). 2022. https://journals.sagepub.com/doi/full/10.1089/jwh.2021.0191
- Prespecified and Integrated Subgroup Analyses from the RECONNECT Phase 3 Studies of Bremelanotide. J Womens Health (Larchmt). 2022. https://pubmed.ncbi.nlm.nih.gov/35230162/
- Rosen RC, Diamond LE, Earle DC, Shadiack AM, Molinoff PB. Evaluation of the safety, pharmacokinetics and pharmacodynamic effects of subcutaneously administered PT-141, a melanocortin receptor agonist, in healthy male subjects and in patients with an inadequate response to Viagra. Int J Impot Res. https://www.nature.com/articles/3901200
- Diamond LE, Earle DC, Rosen RC, et al. Co-administration of low doses of intranasal PT-141, a melanocortin receptor agonist, and sildenafil to men with erectile dysfunction results in an enhanced erectile response. Urology. 2005. https://www.goldjournal.net/article/S0090-4295(04)01272-5/abstract
- Safarinejad MR, Hosseini SY. Salvage of Sildenafil Failures With Bremelanotide: A Randomized, Double-Blind, Placebo Controlled Study. J Urol. 2008. https://pubmed.ncbi.nlm.nih.gov/18538350/ — Note: This publication is the subject of a formal Expression of Concern from the Journal of Urology (2023; doi 10.1097/JU.0000000000003117) over data-integrity questions and is not presented here as reliable evidence.
- National Institute of Diabetes and Digestive and Kidney Diseases. Bremelanotide. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. NCBI Bookshelf NBK573221. https://www.ncbi.nlm.nih.gov/books/NBK573221/
- Spana C, Jordan R, Fischkoff S. Effect of bremelanotide on body weight of obese women: Data from two phase 1 randomized controlled trials. Diabetes Obes Metab. 2022;24(9):1918-1927. PMID 35603902. https://pmc.ncbi.nlm.nih.gov/articles/PMC9314948/